
Jeffrey A. Hall, MD; Michael D. Peters, MD; Peter A. Hilger, MD
Preservation of the middle nasal vault has increasingly become a topic of interest and concern in rhinoplasty. Modification of the nasal dorsum with traditional techniques may create unfavorable cosmetic results and adverse functional sequelae due to collapse of the middle nasal vault. Nasal dorsal reduction invariably involves separating the upper lateral cartilage (ULC) attachments from the dorsal septum. A number of procedures are used to reestablish the width of the middle nasal vault and competence of the internal nasal valve. Spreader grafts are the most frequently used technique. Although these grafts reliably preserve the middle vault, dorsal irregularities may result. Alternative techniques, such as suture suspension of the ULCs to dorsal onlay grafts or direct suturing of the ULCs to the septum, may pose similar problems. We have found that a modification of the Skoog technique for dorsal hump reduction preserves both a favorable aesthetic contour of the middle nasal vault and proper function of the internal valve. This procedure involves removal of the osseocartilaginous dorsum en bloc. The nasal dorsum is further reduced; the removed portion of nasal dorsum is sculpted and then replaced anatomically. Once a favorable position is found for the native dorsal graft, the upper lateral cartilages are resuspended to the graft with suture fixation. The dorsal segment thus acts as a dorsal onlay spreader graft, reestablishing a natural dorsal contour and preserving the middle nasal vault. We can avoid osteotomies in patients with an appropriate preoperative width of their bony base while correcting the open roof with the replaced dorsal segment.
Arch Facial Plast Surg. 2003;5:251-255
The goals of preserving normal nasal function and controlling the aesthetic outcome following rhinoplasty have always presented challenges for the facial plastic surgeon. In particular, the preservation or reconstruction of the middle nasal vault and internal nasal valve after dorsal hump reduction has evolved through several techniques. The classic technique of dorsal reduction described by Joseph entailed dorsal hump removal followed by lateral osteotomies and infracture of the lateral nasal walls to close the resultant “open roof” deformity.1 However, the subsequent narrowing of the bony pyramid and medialization of the upper lateral cartilages could result in middle nasal vault narrowing and internal valve collapse, leading to significant nasal obstruction and a poor aesthetic outcome.
Several techniques have been developed since Joseph’s description to preserve or reconstruct the middle nasal vault and internal valve in the setting of dorsal reduction. These techniques include the “pushdown” technique,2 traditional spreader grafts,3 and onlay spreader grafts.4 Tord Skoog5 described a technique of dorsal hump removal and reconstruction using the resected dorsal segment after modification. The cartilaginous and bony dorsum are removed en bloc, contoured to achieve adequate dorsal reduction, and replaced as a free graft. Skoog reported improved dorsal contouring compared with Joseph’s technique. Skoog’s description did not address any functional considerations.
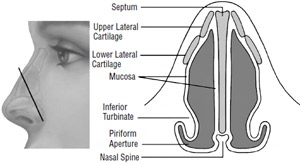
FlG. 1.Internal nasal valve. The valve region is defined by the nasal septum medially, the upper lateral cartilages and piriform aperture laterally, and the anterior head of the inferior turbinate and nasal floor inferiorly..
We describe a modification of Skoog’s technique combined with an open rhinoplasty approach that has been practiced by the one of us (P.A.H.) on selected patients for the last 2 decades. The technique accomplishes simultaneous dorsal reduction, open roof correction, preservation of the middle nasal vault, and natural contouring of the nasal dorsum to achieve excellent functional and aesthetic results without the need for osteotomies.
NASAL VALVE ANATOMY AND PHYSIOLOGY
The internal nasal valve, first described by Mink6 in 1903, plays a key role in the patency of the nasal airway. The nasal valve region is the narrowest portion of the respiratory passage. It is defined as the area bounded by the nasal septum medially, the upper lateral cartilages and piriform aperture laterally, and the anterior head of the inferior turbinate and nasal floor inferiorly (Figure 1). The nasal valve angle is the angle between the septum and upper lateral cartilages and normally ranges from 10° to 15° in the leptorrhine nose; the entire valve region cross-sectional area averages 55 to 64 mm.2,7,8
The nasal valve is the principal regulator of upper airway resistance. As air passes through the valve region, it converts from laminar to turbulent flow, allowing maximal humidification and filtration to occur.9 Airway resistance through the valve area is dependent on its cross- sectional area, as described by Poiseuille’s law, with resistance being inversely proportional to the radius of the cross-sectional area to the fourth power. Roithmann et al10 have demonstrated in patients the dramatic effect of small changes in valve area on nasal resistance by correlating rhinometric (cross-sectional area) and rhinomanometric (nasal resistance) measurements at the nasal valve.
The patency of the nasal valve can be described in a static and dynamic state. In the passive state without inspiration, patency is determined by the resting anatomic relationship of the cartilaginous and soft tissue structural elements of the internal valve. During active inspiration, the valve area is susceptible to collapse due to negative transmural pressure. Dynamic valve patency is determined by the ability of the cartilaginous frame- work and contraction of the nasal musculature to counter these collapsing forces.
Abnormalities affecting the septum, upper lateral cartilages (ULC), turbinates, or muscular and mucocutaneous tissues can cause significant valve obstruction. The most common cause of nasal valve obstruction is acquired deformity secondary to trauma, followed by sequelae of rhinologic surgery.11 Grymer12 demonstrated a 22% decrease in cross-sectional area at the valve region by acoustic rhinometry 6 months after reduction rhinoplasty. It is imperative for the facial plastic surgeon to possess thorough knowledge of nasal valve anatomy and the techniques to prevent long-term morbidity following rhinoplasty.
TECHNIQUE
Between 1980 and the present, one of us (P.A.H.) performed the following modified Skoog technique on selected patients who required dorsal reduction of a primarily cartilaginous dorsal hump. The technique was not used on patients with a primarily bony dorsal hump; in these patients a standard reduction with osteotomies was performed with spreader grafts if indicated.
In the modified Skoog procedure, a standard open rhinoplasty approach with transcolumellar and marginal incisions is used. The soft tissue covering is elevated in supraperichondrial and subperiosteal plane. The anterior septal angle is exposed. Mucoperichondrial flaps are elevated along the nasal septum. Junctional tunnels are developed to free the mucosal attachments from the medial aspect of the upper lateral cartilages and nasal bones. Prior to dorsal reduction, any necessary tip con- touring or repositioning is completed. This sequence is important in establishing the aesthetic balance between the tip and the radix.
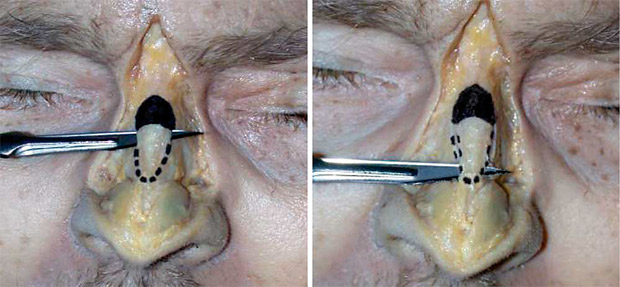
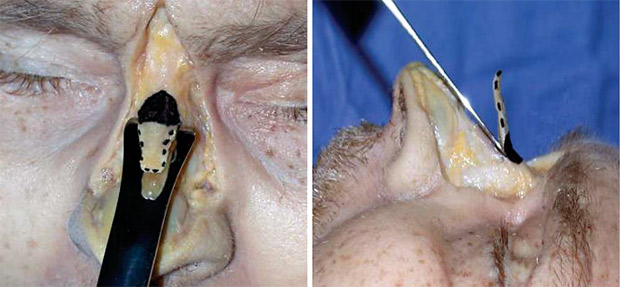
Once the appropriate amount of dorsal reduction is estimated, a No. 11 blade is held at the bony-cartilaginous junction of the dorsum in the horizontal plane of the intended dorsal reduction. The blade is advanced through the cartilaginous dorsum just caudal to the bony junction, transecting the upper laterals and the cartilaginous septum. The blade is then advanced caudally in the plane of reduction to excise the cartilaginous portion of the hump down to the anterior septal angle, leaving it attached to the nasal bones (Figure 2). A 10-mm Rubin osteotome is then inserted under the cartilaginous segment, and the bony dorsum is reduced in the desired plane, removing the entire bony-cartilaginous dorsum in 1 segment (Figure 3). The segment is then modified by removing the septal remnant from its undersurface (Figure 4). This achieves flattening of the segment at the bony-cartilaginous junction, and also prevents displacement of the segment off the midline when placed back into position.
The bony dorsum is further reduced with a rasp, and the dorsal septum and dorsal edges of the upper lateral cartilages are further resected to accommodate replacement of the dorsal segment while achieving the desired hump reduction. This is performed gradually, with repeated replacement of the dorsal segment and redraping of the soft tissues to reassess and prevent overreduction.
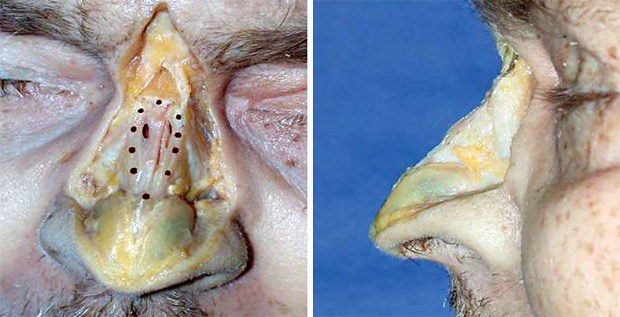
The upper lateral cartilages are then suspended to the lateral edge of the cartilaginous segment with 5-0 polydioxanone suture; a minimum of 2 sutures on each side are required for adequate stabilization. The caudal end of the segment is also secured to the anterior septal angle in the midline or to the cephalic edge of the lower lateral cartilages (Figure 5). Sufficient dorsal reduction, preservation of the middle nasal vault, and correction of the open roof deformity should all be achieved (Figure 6 and Figure 7). After closure, Steri-Strips (3M, Minneapolis, Minn) and a rigid splint are applied and remain until 1 week postoperatively.
RESULTS
One of us (P.A.H.) has refined the described technique over the last 2 decades. We report the results of 22 patients operated on during an 18-month period in 2001 through 2002. Follow-up has been at least 9 months for all patients.
One complication related to the dorsal reduction occurred in our series. A patient presented several months postoperatively with a visible ridge at the lateral aspect of her dorsal segment at the junction with the upper lateral cartilage. She had no complaints of nasal obstruction. The patient underwent revision with an endonasal approach by shaving the ridge through an intercartilaginous incision.
No patients had nasal obstruction secondary to internal valve collapse. Assessments of the nasal airway patency were subjective; no objective measurements of nasal airflow or resistance were performed. All patients had adequate dorsal reduction without postoperative mal- positioning or resorption of the dorsal segment. Proper middle nasal vault width was achieved in all patients. Natural-appearing dorsal aesthetic lines were also pre- served (Figure 6).

COMMENT
A trend in aesthetic rhinoplasty over the last several decades has been to limit resection in favor of realignment and reshaping to preserve normal nasal anatomy and function. In addition, more emphasis also has been placed on the importance of the internal nasal valve and the middle nasal vault in maintaining the nasal airway. Since Joseph’s classic descriptions of osteotomies in the early 1900s,1 several rhinoplasty techniques have been developed to preserve the middle vault, particularly when performing a dorsal hump reduction.
In 1954, Cottle2 described an osteotomy technique of dorsal reduction that preserved the nasal roof and the internal valves. This pushdown technique entailed lateral osteotomies and resection of an inferior strip of septum, which allowed for complete mobilization of the bony and cartilaginous pyramid without dorsal resection. The pyramid could then be pushed posteriorly, into the piriform aperture, reducing the dorsal profile while preserving the nasal valve angle. However, the amount of dorsal reduction attainable with this technique was limited, and it did not gain wide acceptance.


Sheen3 originally described the use of spreader grafts to reconstruct the middle nasal vault. He stressed the importance of middle vault reconstruction when reducing the dorsum, especially in patients with short nasal bones, flaccid upper laterals, or thin skin. Failure to do so could result in upper lateral cartilage collapse, narrowing of the middle vault, and a chevron deformity at the caudal end of the nasal bones. The technique described a “sticklike” cartilaginous graft to be placed endonasally along the dorsal edge of the septum to widen the middle vault roof and increase the valve angle.
Constantinides et al13 demonstrated that spreader grafts result in a long-term objective improvement in nasal valve resistance measured by plethysmography. Alsarraf and Murakami4 described a method of simultaneous dorsal and internal valve reconstruction for type 2 saddle deformities. This onlay spreader graft is similar to our technique except it uses septal or conchal autologous cartilage instead of the resected dorsum. The dorsal onlay spreader graft spans from the nasal bones to the anterior septal angle to straddle the depressed nasal dorsum. The upper lateral cartilages are separated from the caudal septum and sutured to the lateral aspect of the onlay graft to open the nasal valve and provide appropriate aesthetic dorsal width.
The modified Skoog dorsal reduction described herein achieves the following goals: adequate dorsal reduction, correction of any open roof deformity, preservation of the middle nasal vault, and natural contouring of the dorsum. Precise reduction is attained by further resection of the cartilaginous and bony dorsum after the segment is removed. Repeated conservative resection with replacement of the graft and redraping of the soft tissues to assess for adequate reduction are important technical points to achieve the proper amount of reduction. Fixation of the upper lateral cartilages to the dorsal segment prevents middle vault and internal valve collapse seen with traditional reduction rhinoplasty. Using the na- tive segment to reconstruct the dorsum maintains the natural reverse hourglass contour of the dorsum. The natural dorsal aesthetic line may be more difficult to achieve with spreader or onlay grafts, especially in patients with thin skin.
This technique is ideally suited for patients with short nasal bones, a primarily cartilaginous dorsal hump, thin dorsal skin, and limited deviation of the nasal dorsum. This group of patients is similar to the population that Sheen3 originally described as benefiting from spreader grafts (short nasal bones, flaccid upper laterals, or thin skin). These patients are predisposed to middle vault col- lapse after dorsal reduction, osteotomies, and infracture. Our technique is well suited for patients with a dorsal hump and an appropriate or narrow width to their bony base because we eliminate the need for osteotomies to close the open roof deformity.
In conclusion, the described modification of the Skoog dorsal reduction achieves excellent functional and aesthetic results. Adequate dorsal reduction is achieved, any subsequent open roof deformity is addressed, the middle nasal vault and valve region are preserved, and natural contouring of the nasal dorsum is achieved. Our series has shown excellent long-term results with minimal complications.
Accepted for publication August 6, 2003.
This article was presented at the annual meeting of the American Academy of Facial Plastic and Reconstructive Surgery; September 19, 2002; San Diego, Calif.
Corresponding author and reprints: Peter A. Hilger, MD, 5050 France Ave S, Suite 150, Edina, MN 55410.
REFERENCES
- Aufricht G. Joseph’s rhinoplasty with some modifications. Surg Clin North Am. 1971;51:299-316.
- Cottle MH. Nasal roof repair and hump removal. Arch Otolaryngol. 1954;60: 408.
- Sheen JH. Spreader grafts: a method of reconstructing the roof of the middle nasal vault following rhinoplasty. Plast Reconstr Surg. 1984;73:230-237.
- Alsarraf R, Murakami CS. The saddle nose deformity. Facial Plast Clin North Am. 1999;7:303-310.
- Skoog T. A method of hump reduction in rhinoplasty: a technique for preserva- tion of the nasal roof. Arch Otolaryngol. 1966;83:283-287.
- Mink PJ. Le nez comme voie respiratory. Presse Otolarynol (Belg). 1903:481-496.
- Bridger GP. Physiology of the nasal valve. Arch Otolaryngol. 1970;92:543-553.
- Masing H. Experimentelle untersuchengen uber die Stromung im nasenmodell. Arch Klin Exp Ohren Nasen Kehlkopfheilkd. 1967;189:59-70.
- Wei JL, Remington WJ, Sherris DA. Work-up and evaluation of patients with nasal obstruction. Facial Plast Clin North Am. 1999;7:263-278.
- Roithmann R, Cole P, Chapnik J, et al. Acoustic rhinometry, rhinomanometry, and the sensation of nasal patency: a correlative study. J Otolaryngol. 1994;23: 454-458.
- Kasperbauer JL, Kern EB. Nasal valve physiology: implications in nasal surgery. Otolaryngol Clin North Am. 1987;20:699-719.
- Grymer LF. Reduction rhinoplasty and nasal patency: change in the cross- sectional area of the nose evaluated by acoustic rhinometry. Laryngoscope. 1995; 105:429-431.
- Constantinidines MS, Adamson PA, Cole P. The long-term effects of open cos- metic septorhinoplasty on nasal air flow. Arch Otolaryngol Head Neck Surg. 1996; 122:41-45.