
ROBERT H. MAISEL, M.D.,
PETER A. HILGER, M.D.,
GEORGE L. ADAMS, M.D.,
Minneapolis, MN
ANTHONY M. GIORDANO, M.D.,
Richmond, VA
ABSTRACT
Forty-five patients were evaluated for reconstruction of the mandible. Thirty-four patients has a particulate cancellous bone and marrow (PCM) crib graft placed. Thirty of 34 were successful at the primary operation producing a success rate of 88%. By using secondary procedures all 33 patients repaired to date have been rehabilitated. A dynamic bendable defect bridging plate with cancellous cortical graft (DBDB plate with CCG) was used in 7 patients, 4 of whom had tumor surgery and 3 of whom were operated and after trauma to the anterior mandible. All 7 cases were successfully rehabilitated in achieving a stable, functioning mandibular arch.
An osteomyocutaneos flap was planned to reconstruct the anterior mandible in 4 cases; 1 in this group was not reconstructed. The PCM graft has been our first line approach to the mandibular non-union but with experience we are beginning to rely on the DBDB plate with CCG for large bony defects after both trauma and secondarily after tumor surgery. When indicated, the osteomyocutaneos flap has been eminently successful in restoring function and form in the tumor patient.
Rebuilding the interrupted mandibular arch has always merited high level of attention from reconstructive head and neck surgeons. The bony interruption may be due to a non-united fracture subsequent to osteomyelitis, surgical resection, or due t abrupt traumatic loss of bone. These varying etiologies all dictate that the interested surgeon consider rebuilding the mandible.
Fracture bones heal by a natural process where bone crosses the defect under conditions of Immobilization, direct apposition of bony fragments, and protection from infection ad well as coverage by soft tissues. In most adults, bony union of the mandible will occur under the above condition after 6-8 weeks. Failure to unite at this point results in a delayed or non-union. Should a delayed union not heal with time and further conservative treatment, it would the defined as a non-union. Osteomyelitis of the bone causes absorption and loss of the normal bony architecture and separates infected fragments, preventing their apposition and healing by bony union. Similarly, an explosive injury, which throws fragments out of the body or leaves devitalized bone, will require replacement of the missing or defective osteoid fragments.
Many of these patients are otherwise healthy, often young and active, and need an intact mandibular arch for cosmesis, mastication and best communication. Since the are usually in good general medical condition, massive reconstructive efforts can be comfortably undertaken once several general surgical principles are met.
The mandibular segment which must be sacrificed to safely resect and intraoral carcinoma with adequate tumor margins has been less aggressively reconstructed than the non-united mandible after trauma. Among he reasons for this are the general debility of the patient, or the prior use of radiotherapy of planned combined therapy in conjunction with the surgical procedure. Further, the risk of disabling the oral cripple by additional local surgery in area with inadequate soft tissue coverage has swayed surgeons away from further reconstructive procedures.
Over the past 10 years, 3 different techniques have been user reconstruct the mandible at the university of Minnesota Hospitals. These techniques involve combinations of alloplastic autogenous implants to maximize the success of such rehabilitative surgery.
METHODS AND MATERIALS
PCB Crib Graft. From January 1973 through December 1982, 30 patients with traumatic interruption of the mandibular arch and 4 patients who had full thickness resection of the mandible at the body and symphysis during treatment of an oral neoplasm were candidates for mandibular reconstruction. A crib graft containing particulate cancellous bone and marrow (PCM) was used in all but 3 cases. Three patients had a crib placed without bone. Angle and ascending ramus resections are not reconstructed at institution after tumor surgery, since the disability it produces has not been significant.
The technique used is similar to that described by Boyne and modified as described by Giordano and by Maisel. The specifics of the technique can be found in the above cited references. The important aspects of the method to highlight are the use of a Sampson titanium crib (tray), with cancellous bone and marrow, both harvested from the ipsilateral iliac crest. Donor tissue is obtained by fracturing the cortical cap of the iliac done leaving the sartorius and other muscles attached to the anterior superior spine and used chisel, gouge and curette to harvest the bone which is preserved in a blood filled container. When less bone is required, particularly in the male and the female where the pelvic bone is thick, a Clower drill which takes a direct core of cancellous bone and marrow has been used.
Titanium is preferable to the chrome-cobalt (Vitallium®) cage because the former is more malleable. The metal crib is secured by at least 3screws of material identical to the cage, (titanium) to minimize electrolytic osteolysis. These screws, 3 on each fragment of mandible, are placed after a drill hole is formed by hand and not by power drill (to prevent osteitis). They are placed by preference, with 2 of the screws at 90° to each other in each proximal and distal mandibular stump. We do not user a Millipore filter and have not in any of our cases. The oral mucosa must not be penetrated in preparing the soft tissue bed as infection will likely occur. A large rent of the oral mucous membrane overlying the mandible should be grounds for abandoning the procedure until a second occasion; therefore, the graft is not harvested until the recipient site is prepared.
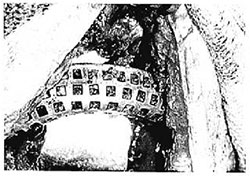
Fig. 1. The chips of particulate cancellous bone and marrow tightly packet fill the cage of titanium. This patient had secondary reconstruction of an angle to angle resection of a floor of mouth carcinoma.

Fig. 2. The DBDB plate with CCG is seen with 3 screws applied to each mandibular stump. A screw penetrating the cortical plate of the graft is not visible, but is present and secures the bone to the burr.
External fixation using the Morris biphase or internal fixation using intermaxillary wiring in the fully dentulous patient has been used to immobilize the mandible and to prevent motion of the tray which is filled and tightly packed with chips of cellous bone and marrow (Fig. 1).
DBDB Plate Technique. The second technique we have used is similar to that employed by the Swiss surgeons. It involves securing 1 to 2 cm fragments of cancellous iliac bone with a cortical cap on each fragment. These are secured to a malleable stainless steel bar. The recipient bed is prepared and a 3-dimensional bendable defect bridging plate (3-DBDB plate) is secured to the mandible by at least 3 screws on each side (Fig. 2). The screws engage both cortices and are placed into hand-drilled holes. The donor bone is then placed in the concavity of the arch and each large fragment is impacted by a screw through the cortical cap to hold it in position. Spiessl and his group have described using 5000 kp/cm2. This then creates a form identical to that of the missing mandibular bone. This equipment is not yet commercially available in the United States.
The technique as we have used it has been performed in 7 patients from January 1978 through December 1982. Four of these patients have had high dose radiation for cure of oral carcinoma with subsequent obvious radiation effect to the local tissues of the skin, the bone, and the interposed soft tissue. The radiation had been completed 1 to 3 years preimplant in all 4 cases. These 4 patients all had been operated on for cure and had no evidence of recurrent tumor when reconstructed.
Osteomyocutaneous Flap. In 4 patients with large intraoral carcinomas, which required mandibular resection of the entire anterior arch in 2 patients, and the resection of the body and ramus in the other 2, a pectoralis major osteomyocutaneous flap was prepared. All patients had an intraoral soft tissue defect was enough to require a flap to rehabilitate the oral cavity. Planned mandibular reconstruction, using the 5th rib elevated and maintained in continuity to the pectoralis muscle, was performed completely in 3 patients.
The flap was used for reconstruction in the manner described by Cuono and Ariyan* and Maisel, with elevation of the flap and skin incisions drawn as indicated by Maisel and Liston. An external biphase was applied in all cases after sculpting the rib to fit the defect and using #28 gauge wire in a figure of eight pattern to secure the rib to the mandibular stump. The patients were maintained in external fixation for a period of 12 weeks at which time a panorex x-ray was taken (Fig. 3). Review of the x-ray as well as clinical examination of the patient for absence of pain and mobility as well as a visible healed intraoral skin flap recommended removal of the biphase. Dentures were not permitted until 1 year post-reconstruction.
RESULTS
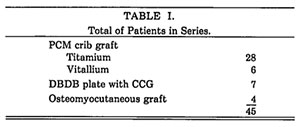
Forty-five patients comprise this series of mandible reconstruction (Table 1). Thirty-one patient had a particulate cancellous bone marrow (PCM) graft placed in a crib Three of the tumor patients had a titanium crib placed, at their primary operation, without any bone chips. Twenty-eight of the cribs were made of titanium; six were of Vitallium®. Two of empty cribs were applied as a spacer at the time of cancer resection with the plan to fill the crib with marrow and cancellous bone at a second stage.

Fig. 3. Panorex x-ray of a patient with an osteomyocutaneous flap. The x-ray is taken 12 weeks after reconstruction and confirms the clinical impression of bony union. The Biphase shown on the x-ray was removed and the patient has a stable mandibular arch.
The other patient had resection of a large benign tumor requiring removal of the condyle and a titanium crib with a metal condyle was applied without filling the cage. Of the 31 patients who had a bone graft, 27 of these were successfully reconstructed primarily with radiographic evidence of bone growth, or intraorally palpable hard tissue filling the cage and extending superior to it. One such patient had firm fibrous tissue conforming to the shape of the cage. This was confirmed on exploration of the neck for recurrent carcinoma. Four patients had rock hard bone when the cage was removed for the symptom of cold intolerance in 1 and for intraoral exposure and pain in the other3; 2 patients who were primary failures due to instability of the cage and bone graft were successfully regrafted. Another patient had intraoral exposure with sequestration of the grafted bone necessitating intraoral removal of the bone from the cage and secondary removal of the cage. This was replaced by a bar of the type described below (a 3 DBDB plate without bone graft)). A recent case has failed and the titanium cage has been removed. This patient is being stabilized with a biphase for a period of 6 months until a second grafting will be attempted.
One patient has persistent intraoral exposure of the empty cage with no others difficulties. Thus far 29 of 30 patients who were repaired post-trauma were successfully rehabilitated and have a stable and intact mandibular arch. All 4 patients repaired post-tumor resection have successfully rehabilitated although 2 of these patients had recurrent tumor within 2 years of completing their treatment.
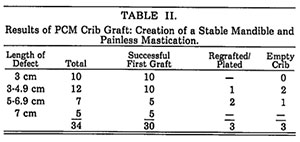
Four criteria were applied to evaluate the results of the PCM technique. Criteria for success include: 1. a non-moving mandibular fragment incorporated into the bony arch, 2. satisfactory occlusion, 3. the ability to crew, and 4. the ability to swallow and articulate. Table II shows an 88% success rate (30of 34 patients) in the ability to stabilize the mandible with this single procedure. We are able to obtain satisfactory and painless mastication. With secondary procedures, success has been achieved in all but one patient. Dental occlusion is much less secure and critical evaluation suggests a success rate no greater than 75% in achieving pre-injury occlusion pattern in the dentulous patient. Many of these patients have not been able to wear dentures over the grafted mandible and have been discouraged from this whenever difficulties have arisen.
From this series it appears that bony discontinuity in the parasymphyseal and symphsyseal area represents the greatest liability in the success of the PCM crib graft. (Three of the failures involved injuries to this region.). Of 7 patients treated with a 3-DBDB plate with cancellous cortical graft (CCG), all mandibles were successfully restored as a firm bony continuity. The metal plate remains implanted in all 7 patients. Of the 4 patients who were repaired secondarily after tumor resection, 3 were edentulous. Two of these have returned to wearing dentures, providing them with satisfactory occlusion and mastication. Most of the patients in our series have insufficient teeth to judge occlusion accurately.
All patients whose bone loss was due to trauma have been returned to their pre-injury occlusion by a two stage procedure which used intermaxillary fixation and external bar appliances (Morris biphase) to maintain the pre-injury anatomic relationships in stage 1 of their reconstruction. This allowed healing of the contaminated wound and subsequently permitted application of the 3-DBDB plate with CCG. The 4 patients operated on for large intraoral carcinoma with osteomyocutaneous flap reconstruction included 2 with resection of the ipsilateral body and parasymphysis and 2 patients in whom the cancer operation necessitated resection of the entire anterior mandibular arch, including the entire body unilaterally and resection to the body on the side contralateral to the major tumor bulk. The bone defect measured 5-9 cm in each.
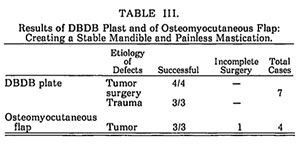
The operation was completed successfully in 3 patients and in 1 case was completed without using rib in a patient with a lateral mandibular defect (Table III). This was due to technical difficulty in maintaining the rib and flap in continuity and it was elected to reconstruct this patient’s mandible at a second operation. This procedure was successful in all 3 patients where it was completed. The fourth patient had a successful rehabilitation of the oral cavity, but was left with discontinuity of the mandibular stumps.
Two patients including the patient with an unrepaired mandibular defect died of recurrent carcinoma in the neck and at the base of the skull. The other 2 patients are alive and well, 18 and 12 months respectively and the first has been fitted for dentures.
DISCUSSION
Theoretic and practical indications for reconstruction of bony defects are most intense in the mandible. While this is not a weight-supporting bone it is frequently in motion: and, because of this constant stress, the prosthesis or graft may become mobile and eventually become infected or rejected. Should the Prosthesis site become contaminated the bone may either become exposed, sustain osteomyelitis, extrude or require removal. However, if a sufficient interval has occurred using the techniques described above, bony union will have taken place and the graft is no longer at risk. The support structure of metal may the safely be removed.
Our failures using the particulate cancellous bone and marrow graft in a tray of titanium or Vitallium® have been infrequent and these failures to achieve bony union have been related to errors in technique. They also relate in large measure to the location on the mandible. The symphyseal and parasymphyseal areas area greater risk because of their poorer blood supply, increased stress from muscle pull at the mentum and relatively inadequate soft tissue coverage. The tenets described under Methods and Materials include ensuring adequate soft tissue with healthy blood supply before beginning the grafting procedure. The operation should be avoided in the face of lacerations to the mucous membrane which are either not repaired or which are difficult to repair as a water tight seal.
The empty crib is less likely to be successful since subsequent removal due to pain, mobility, or exposure will again leave and interrupted mandibular arch. Failures can be reoperated on with little compromise due to previous attempts. In essence these grafts fail to heal for the same reasons that mandible fractures fail to heal, inadequate fixation, inadequate soft tissue coverage, intraoral sepsis and grafting in the face of infection. Lawson and Biller described 18 delayed reconstructions of the mandible tumor resection using the titanium mesh tray. They did not delineate their criteria for success or the location of the defect but reported an 83% success rate. Hahn and Corgill reporting in 19369 had a 79% success rate using Vitallium® cage in 60 cases. They similarly were operating primarily in an older population where the mandible loss had included soft tissue in the course of cancer resection.
We therefore, feel that the crib graft gives us a reliable result using autogenous bone in a somewhat malleable tray which can be made to conform to the shape of any mandible. Presently we have difficulty when the condyle needs to be replaced, as our preferred commercially available metal cage does not have a condyle.
Despite the excellent results using this technique, we have begun to try the DBDB plate with CCG which has been uniformly successful in our small series and has been utilized in higher risk patients including those who had high dose radiation with resultant obvious soft tissue injury. In the latter patients, a regional rotation flap was required as a staged procedure preceding the graft implant in some patients. All seven cases where the graft has been used have been successful.
It has been theorized that cancellous bone in a titanium cage has only a 50% opportunity to be exposed to tissue fluids compared to 80% exposure with dynamic bendable plate (a rib flap should be 100% exposed to vascular nourishment). Spiessl’s experience with compact cancellous bone further indicates that of the implanted tissue increases by 20% the size of the graft and, therefore, the amount of osteogenic material. There is subsequent absorption of 25% to 40% of such tissue in final healing.
Utilizing the pectoralis major myocutaneous flap to reconstruct the mandible in conjunction with an applied rib graft has been successful in all there instances where the operation has been completed. The technique for securing the donor graft is not very dissimilar from that of other reporters. Rib instruments are used to separate the rib from the pleura and attempt to maintain the pleura intact. The posterior periosteum is taken with the rib and the rib is cut at its chrondocostal junction and also laterally giving a length of rib sufficient to fir the defect. The periostium of the rib is deliberately sutured to the soft tissue of the flap to prevent shearing the rib from the muscle attachment.
Medgyesi reporting in 1973 described and extensive vascular network connecting the muscle, bone and periosteum using the goat as an anatomic model. His speculation was that the vascular connection noted in the osteomuscular flaps was better than in those bones transferred and attached only by skin pedicle. He explained this by the observation that muscle and bone are both mesodermal in origin. The animal model may explain the success of this compound flap in rapidly vascularizing the rib and joining it by a bony union to the mandible.
Cuono and Ariyan were the first to describe combining the concept of the myocutaneous flap with the free rib graft and using it to reconstruct the mandible. They confirmed their success by bone biopsy after tetracycline labeling and further supported their thesis by using a technetium scan of the bone. Lawson and Biller were successful in 3 or 5 cases using immediate reconstruction after tumor surgery. A larger reported series by Bell and Baron while not carefully tabulated suggests that 10 of their 14 patients were successful in this type of reconstruction. Their indications for the soft tissue flap are clearly delineated in the article.
Evidence for satisfactory healing in our cases has been by radiography demonstrating bony union with evidence or calcification in the rib after 12 weeks of immobilization. Utilizing clinical signs such solidarity of the mandible and manipulation and absence of pain at the juncture of mandible and rib further suggested a good bony union.
In the patients who have had the osteomyocutaneous flap, a large regional flap to reconstruct the soft tissue defect was necessary as part of the primary operation and reconstruction. Adding rib to the flap increased the chance for a one-stage reconstruction of the patient, eliminating the need for secondary operation. This produced a more rapid rehabilitation of the oral cavity. The additional time to dissect and place the rib was less than 30 minutes.
There have been no failures in this small series and it is anticipated that any failure will result in a temporary fistulization through the juncture of myocutaneous flap and recipient mucous membrane or skin with good resolution by careful wound healing techniques. Such a complication may require a small secondary procedure to remove the bone flap and would leave us in the usual circumstance with a soft tissue flap and non-united mandibular fragment secured in position by external fixation. If such a failure occurs it would not prevent mandibular reconstruction in 6-12 months using the DBDBD plate with CCG. Postoperative radiation therapy to the mandible after ostemyocutaneos reconstruction has not had adverse effects. Two of the 4 patients who entered this section of the study have died of recurrence in the neck less than 2 years after the diagnosis. They were initially staged as T3N2 floor of mouth cancer.
The essential principles which must be adhered to include the following:
- Adequate soft tissue coverage must be available either primarily or through rotation flaps. This can be staged previous to the reconstruction in the first two described techniques and can be applied during the reconstructive effort utilizing the osteomyocutaneous flap.
- Graft exposure either intraorally or externally risks loss of the graft.
- When necessary to stage the procedure, the mandibular fragments are maintained in anatomic position by external fixation.
- The soft tissue is reconstructed by placing tissue without tension and replacing any missing tissue with regional flaps, rather than trying to close tissue in a non-anatomic position. After an adequate period of healing to ensure no infection will ensue, a bone graft can be applied.
SUMMARY
The aim of the reconstructive surgeon addressing the mandible is to achieve a stable bony arch which produces painless mastication without motion of fragments, and we have found excellent and virtually equal success using the three techniques of mandibular crib graft consisting of a titanium tray with cancellous bone and marrow inserted, dynamic bendable defect bridging plate with cancellous cortical graft, and in appropriate patients utilizing an osteomyocutaneous pectoralis flap based on the fifth rib anteriorly.
BIBLIOGRAPHY
- Mathog, R.H. and Boies, L.R.: Nonunion of the mandible. LARYNGOSCOPE, .5:908-920, 1975.
- Foster, C. A., Meyerhoff, W. L. and Maisel, R, H,: Shotgun Wounds of the Face. In: plastic and Reconstructive Surgery of Head and Neck. Chapter 7. Leslie Bernstein, M.M., D.D.S. (Ed.). Grune and Stratton, Inc., New York, NY. Pp. 37-45, 1982.
- Boyne. P. J.: Restoration of Osseous Defects in Maxillofacial Defects. J. Am. Dent. Assn., 78:767-776, 1969.
- Giordano, A., Brady, D., Foster. C., et al.: Particulate Cancellous Marrow Crib Graft Reconstruction of Mandibular Defects. LARYNGOSCOPE, 90:2027-2036, 1980.
- Maisel, R. H,: Mandibular Reconstruction. LARYNGOSCOPE, 90:334-336, 1980
- Spiessl, B.: New concepts of Maxillofacial Bone Surgery. Springer-Verlag, Berlin, Heidelburg. New York, pp. 156-166,1976.
- Spiessl, B.: A New Method of Anatomical Reconstruction of Extensive Defects of the Mandible with Autogenous Cancellous Bone. J. Maxillofac. Surg., 8:78-83, 1980.
- Cuono, C. B. and Ariyan, S.; Immediate Reconstruction of a Composite Mandibular Defect with a Regional Osteomusculocutaneous Flap. Plast. Reconstr. Surg.. 65:447-483, 1980
- Maisel, R. H, and Hilger, P. A, and Adams, G. L.: Osteomyocutaneos Reconstruction of the oral Cavity. In press 1983. (Presented at the American Society for Head and Neck Surgery meeting in Palm Springs, CA, March 1983.)
- Maisel, R. H, and Liston, S. L.: combined Pectoralis Major Myocutaneous Flap with Medially Based Deltopectoral Flap for Closure of Large Pharyngocutaneous Fistulas. Ann. Otol., 91:98-100, 1982.
- Lawson, W, and Biller, H, F,: Mandibular Reconstruction: Bone Graft Techniques Otolaryngol. Head Neck Surg., 90:589-594, 1982
- Hahn, G. W, and Corgill, D. A,: Chrome Cobalt Mesh Mandibular Prosthesis. J. Oral Surge. 27:5-10, 1969.
- Medgyesi, S: Observations on Pedicle Bone Grafts in Goats. Vascular Connections Between Soft Tissues and Bones. Scand. J. Plast. Reconstr. Surg., 7:110-115, 1973.
- Bell, M. S. G, and Barron, P. T.: The Rib-pectoralis Major Osteomyocutaneous Falp. Ann Plast Surg., 6:347-353, 1981.
DISCUSSION
JHON M. FREDRICKSON. M.D. (St. Louis, MO): How many of those cases had been irradiated prior to operation?
DR. MAISEL: All of our tumor cases had been irradiated. Three of the dB plates were radiation failures and were resected because of that. One was planned high dose postoperative radiation and was reconstructed two years later.
©2012 Hilger Facial Plastic Surgery