
Steven S. Orten, MD; Peter A. Hilger, MD; Minneapolis, Minn
A 49-YEAR-OLD PATIENT was seen in consultation for evaluation of chronic nasal air- way obstruction. In 1967, he underwent a septorhinoplasty with significant skeletal reduction to improve the form and function of his nose. His airway was worse postoperatively. The patient noted improvement in his breathing with lateral traction on the soft tissues of the cheek. He has inhalant allergies to dust, mold, and pollen. He takes oral antihistamines with only minimal improvement of his breathing. He notes total nasal airway obstruction with sniffing.
Physical examination reveals collapse of the right nasal bone and a deformity at the inferior aspect of the nasal bones at the junction with the upper lateral cartilage (Figure 1 through Figure 3). The anterior nasal spine is deviated to the left. The nasal septum is deviated to the left also. A cotton-tip applicator placed intranasally at the caudal margin of the upper lateral cartilage provides remarkable improvement in the nasal airway
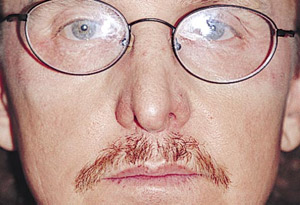
FlG. 1. Frontal view.

FlG. 2. Base view.

Fig. 3. Sky view from above.
SURGICAL SOLUTION
Nasal valve collapse
Nasal obstruction is a common complaint with multiple causes and can often result from several coexisting factors. Reversible and nonreversible factors limiting airflow may be at play. Allergic-, vasomotor-, or pregnancy-associated rhinitis as well as the normal nasal cycle are common reversible causes of airway obstruction. The nonreversible causes are anatomical obstructions, which may be classified as “fixed” or “dynamic” in nature. Examples of fixed obstructions are deviated nasal septum, polyps and neoplasms, nasal stenosis, and nasal valve collapse. Valve collapse may also be dynamic and related to the Venturi effect. As nasal air flows through the narrow valve area, a negative pressure is created, collapsing the structurally weak nose medially. When inspiration becomes expiration, the negative pressure ceases and the nostril lateralizes to its original position. Nasal valve collapse may have components that are fixed, dynamic, or both.
The etiology of nasal valve collapse may be congenital or secondary to trauma, aging, or iatrogenic causes. Nasal valve collapse is not an infrequent complication for the patient complaining of nasal obstruction after rhinoplasty surgery. The nose weakened by a reduction rhinoplasty may result in a decreased cross- sectional area of the nasal valve or the structure may be so weakened that it only becomes apparent when the patient inspires.
The nasal valve has been viewed as 2 valves in series with an internal and external component. The anatomical location of the internal valve corresponds to the area of the caudal upper lateral cartilage, septum, nasal floor, and head of the inferior turbinate. Internal valve obstruction occurs when the upper lateral cartilage col- lapses medially into the airway. Causes of internal valve collapse may be due to loss of tissue resilience with aging or the weakening or narrowing of the structural support of the middle third of the nose during trauma or surgery. Excessive narrowing of the bony vault with osteotomies can medialize the upper lateral cartilage. Dorsal reduction, which detaches the articulation of the upper lateral cartilage from the septum or overresection of the upper lateral cartilage with cephalic trim, can give rise to internal valve collapse. Trauma with avulsion of the upper lateral cartilage from the bony vault can also collapse the middle third of the nose. Nasal vestibular- lining injuries may lead to soft tissue contraction and scar- ring, which creates secondary collapse of the cartilaginous framework or webbing. When internal valve collapse occurs for any reason, the middle third of the nose may appear “pinched” or “hourglass shaped.” The patient may notice that the Cottle maneuver (lateralizing the nostril with a finger on the cheek) results in improved breathing. The lateral wall of the nose at the internal valve may be seen to medialize when the patient is carefully observed during inspiration. This sign is often missed by the clinician if a speculum is used to stent the valves open during inspection.
External nasal valve collapse represents a distal collapse of the nostril opening at the alar margin. This occurs when the nostril openings are narrow, “slitlike,” and weak congenitally; the lateral crura have been weakened by over resection or are cephalically oriented and do not adequately support the alar margin. External valve collapse is usually more obvious, because the flailing alae are more visible than the internal valve during inspiration.
The multiple factors involved in nasal valve collapse often demand multiple approaches. Numerous methods have been described for correction of valve collapse, which attest that no one approach has been universally successful.
The simplest method to relieve nasal valve obstruction temporarily is with the use of prosthetic devices to splint the nasal valve open. Springs taped to the external nose and wire baskets used as dilating splints placed inside the nose provide temporary relief during exercise or sleep but are not socially acceptable in most situations.
The most frequent method used to surgically correct internal nasal valve collapse involves the use of spreader grafts placed between the upper lateral cartilage and septum. This lateralizes the dorsal margin of the upper lateral cartilage and widens the middle nasal vault but only minimally increases the cross-sectional area because the angle of the internal valve is not appreciably affected. Spreader grafts are most effective when the middle third of the nose is “too pinched” and frequently results in greater improvement in the aesthetic appearance of the nose than in improved airflow.1,2 Patients with severe internal or external valve collapse will require other adjunctive procedures to enhance the results of spreader grafts.
A variety of structural cartilage grafts have been advocated to support the weakened lateral nasal wall. Among these, the alar batten graft is commonly used. Grafts are taken from the septum or auricle and placed into precisely positioned pockets or sutured to the point of maximal lateral wall collapse. Batten grafts reinforce the nasal side wall and prevent collapse during inspiration. Battens may change the resting anatomy of the nose if the graft extends to the pyriform aperature and the nasal valve is stented open by suturing the valve cartilages to the graft. Grafts are frequently placed at the junction of the upper and lower lateral cartilage for internal valve collapse and closer to the alar rim for external valve collapse.
Several different suture-suspending and flaring techniques have been described. These techniques may be required when spreader and batten grafts do not sufficiently relieve nasal valve collapse. Park3 describes a vertical mattress-flaring suture placed bilaterally through the caudal aspect of the upper lateral cartilage and tied over the nasal dorsum. This suture gives a lateral flare to the nasal valve and increases the cross-sectional area. Paniello4 places a mattress suture from the point of maximal nasal collapse to the orbital rim through a transconjunctival incision, in this way lateralizing and suspending the nasal side wall. When additional lateralization is needed after spreader and batten grafts have been placed, we have suspended the lateral nasal wall to an absorbable fixation screw (Lactosorb; Lorenz Surgical, Jacksonville, FL) or a nonabsorbable anchor placed in the frontal process of the maxilla. This is performed through an open rhinoplasty approach or a small buccogingival incision. A suspending suture is passed from the point of maximal nasal valve collapse to a screw placed in the maxilla lateral to the pyriform aperture.
Our patient required an integrated comprehensive approach to correct his obstruction. A septorhinoplasty was performed through an open approach. A left spreader graft of septal cartilage was used along with bilateral alar batten grafts harvested from the auricular concha. The spreader graft did not adequately support the internal valve and the batten grafts were added to restore an appropriate airway. The patient was pleased with improvement in form and function.
Numerous other techniques have been described to correct nasal valve collapse. Most of these techniques have merits as well as limitations. Nasal valve collapse, how- ever, can be a complex problem with a variety of causes that may require the facial plastic surgeon to have several techniques in his or her armamentarium to address this problem.
REFERENCES
- Toriumi DM, Josen J, Weinberger M, Tardy ME. Use of alar batten grafts for cor- rection of nasal valve collapse. Arch Otolaryngol Head Neck Surg. 1997;123: 802-808.
- Stucker FJ, Hoasjoe DK. Nasal reconstruction with conchal cartilage: correcting nasal valve and lateral nasal collapse. Arch Otolaryngol Head Neck Surg. 1994; 120:653-658.
- Park SS. The flaring suture to augment the repair of the dysfunctional nasal valve. Plast Reconstr Surg. 1998;101:1120-1122.
- Paneillo RC. Nasal valve suspension. Arch Otolaryngol Head Neck Surg. 1996; 122:1342-1346.
SUBMISSIONS
Residents and fellows in facial plastic surgery are in- vited to submit quiz cases for this section and to write letters to the ARCHIVES commenting on cases presented. Quiz cases should follow the patterns established. See “Instructions for Authors.”
Material for the FELLOW’S PAGE should be mailed to the Editor. Reprints not available.
Downloaded from archfaci.ama-assn.org at University of Minnesota Twin Cities, on 29 February 2012 ©1999 American Medical Association. All rights reserved.