
Philosophical Considerations
Traditional practice in rhinoplasty has tended to rely on resection of the nasal osseocartilaginous framework to achieve aesthetic or functional objectives. Most successes using this approach have proved short lived because the weakened nasal scaffold remaining after reductive surgery often has inadequate strength to withstand the contractile forces of healing. The classic stigmata of an overresected nose, including alar retraction, internal and external nasal valve collapse, midvault collapse, loss of tip support and projection, and unnatural sharp contours such as bossae formation, have become all too familiar to the revision rhinoplasty surgeon. The loss of structural integrity observed in patients who have saddle nose deformity is frequently an iatrogenic complication caused by failure to preserve an adequate dorsal strut at the time of surgery. The resulting pattern of dorsal and middle vault depression, tip over rotation, loss of tip projection, retraction of the columella, and unnatural contours in these patients is disfiguring and functionally crippling. The poor durability of aesthetic outcomes and the progressive functional impairment associated with reductive surgery have provided a major impetus for the development of grafting approaches in rhinoplasty. This article details the role of structural and aesthetic grafting in rhinoplasty with the objective of promoting reproducible and durable surgical outcomes. A review of the various grafting materials available to the rhinoplasty surgeon is followed by a discussion of the relevant anatomy, terminology, and indications for each grafting approach. In keeping with the objective of achieving predictable longterm results, emphasis is placed on the use of autogenous cartilage grafts, which are associated with more favorable outcomes and lower complication rates than other, alternative grafting materials. This topic alone can justify an independent text, and we are sensitive to the constraints associated with this publication. Therefore, we have provided concise descriptions and illustrations of the relevant surgical techniques and appended a detailed bibliography for readers seeking further discussion.
The soft tissue skin envelope and its underlying osseocartilaginous framework are intimately related, together influencing the external appearance and functionality of the nose. In primary rhinoplasty, suboptimal surgical outcomes commonly result from the buckling of a weakened nasal skeleton that lacks sufficient structural rigidity to withstand the contracture forces generated by the healing soft tissue skin envelope. In revision rhinoplasty, the limiting factor in correcting a previously operated nose is frequently the quality, degree of contraction, and lack of elasticity of the soft tissue skin envelope and the intranasal lining.
It is therefore imperative that the surgeon be able to understand and conceptualize the dynamics of postoperative healing while manipulating the nasal framework. Moreover, the surgeon must possess the requisite skill and intellectual dexterity to modify the proposed surgical plan, because distorted anatomy is frequently encountered during surgery. Virtually all techniques designed to provide focal alteration of form or function will have secondary effects in other areas of the nose. The skilled rhinoplasty surgeon anticipates these alterations and adjusts the procedure appropriately.
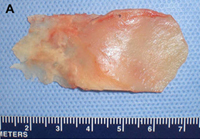
Fig. 1. Autogenous grafting materials. (A)Septal cartilage.

(B) Conchal cartilage.

(C) Costochondral graft.
Conservative resection, framework remodeling, and judicious use of grafts for augmentation comprise the basis for a structural approach to grafting in rhinoplasty. In primary rhinoplasty, major and minor support mechanisms are often weakened by surgical maneuvers. Grafts are used to reconstitute support elements thus compromised and to effect desired changes. In contrast, revision rhinoplasty often involves rebuilding nasal framework in the setting of significant structural deficiency. Excessive resection involving the lower lateral crura, the caudal septum, and the nasal dorsum is often compounded by disruption of other tip support elements. The resulting weakening of the nasal architecture is further exacerbated by scarification of the nasal lining and external soft tissue covering. The surgeon can use appropriately selected grafting techniques to correct problematic anatomy or to protect at risk areas. A systematic approach to grafting makes it possible to achieve lasting improvement in aesthetic appearance and nasal function, always taking care not to compromise function in the pursuit of aesthetic gain.
Graft Materials
Various grafts and implants are available for use in primary and revision rhinoplasty. Although no ideal grafting material exists, with appropriate graft selection and sound surgical technique, dependable outcomes can be achieved. Grafts can be broadly categorized into autogenous, homologous, and alloplastic types. Injectable agents such as hyaluronic acid fillers are occasionally used for refinements.
Autogenous Grafts
Autogenous grafts are harvested from the patient and include cartilage, bone, and various soft tissues, such as perichondrium and temporalis fascia. Autogenous cartilage is the structural grafting material of choice because of its ease of carving and reliable longterm outcome, with low rates of infection, resorption, and extrusion. Autogenous grafts also avoid the potential risk for an immune response or viral contamination. Cartilage grafts are useful for providing structural scaffolding and creating contour. Representative septal, auricular, and costochondral grafts are shown in Fig. 1. When crushed, cartilage remains viable and supports the growth of surrounding cartilage.
Septal cartilage is the most commonly used grafting material in primary rhinoplasty, owing to its straightforward harvest and lack of functional or cosmetic donor site morbidity. Furthermore, septal cartilage is particularly versatile in grafting and has reliable longterm results. It is useful for spreader grafts, columellar struts, alar battens, dorsal augmentation, and alar rim grafts. Septal cartilage can also be crushed to provide volume augmentation or to soften contour transitions. When harvesting septal cartilage, it is important that a 1.0to 1.5-cm L-shaped caudal and dorsal strut is maintained. Septal cartilage is often limited in the revision rhinoplasty setting. For major revisions, we prefer to harvest cartilage using an open rhinoplasty approach in which bilateral submucoperiosteal and submucoperichondrial flap elevation is combined with division of the upper lateral cartilages. With this approach, the septum and nasal dorsum are ”ouvert au ciel” (open to the sky), achieving unparalleled exposure for diagnosis, harvest of residual structural material, and treatment of structural deformities.
Auricular cartilage is usually harvested for use in revision rhinoplasty when septal cartilage is inadequate. The auricular cartilage is more malleable than septal cartilage and has a curved shape. This curvature and pliability make auricular cartilage a less desirable grafting material for certain purposes, such as when spreader grafts are needed or a thin columellar strut is desired. It is useful to determine preoperatively if one ear is more prominent than the other, because conchal harvest may confer a subtle decrease in the prominence of the donor ear. Alternatively, the surgeon may ask the patient if he or she prefers to sleep on a given side (a ”sleep crease” is often discernible in the preauricular region on this side) and then use the contralateral ear. We prefer to harvest auricular cartilage grafts from a postauricular approach because the dissection is straightforward and the incision is hidden. When the conchal bowl is harvested, care is taken to preserve the antihelical fold and a strut of cartilage projecting from the crus helicis, which divides the concha cymba and concha cavum. These measures avoid deformity of the auricle. The soft tissue dead space of the donor site is eliminated by a Betadine ointment bolster that is secured with through and through 3-0 nylon sutures. The concha cymba has dimensions, contour, and structural characteristics similar to the lower lateral cartilage, making it a favorable donor site for reconstruction of this structure. Composite grafts from this site may prove particularly useful in the correction of alar retraction. The concha cavum has a concave shape that makes it advantageous for tip grafts, alar battens, and dorsal onlay grafts.
Costochondral grafts afford the rhinoplasty surgeon ample grafting material for the structurally deficient nose. Rib cartilage is most likely to be required either after a disfiguring traumatic injury or following overzealous resection during prior reductive rhinoplasty. The excellent quality and quantity of costal cartilage make this the donor site of choice when septal and auricular cartilage is insufficient. The principal disadvantages of rib cartilage are the tendency for warping, the donor site scar and postoperative pain, the potential for rigidity and calcification of the cartilage in the mature patient, and the added operative time. The patient must also be counseled regarding the small, yet well established, risks for infection, hematoma, postoperative splinting, and pneumothorax associated with this donor site. We have found the use of continuous infusion anesthetic pumps with 0.25% bupivacaine to be a simple and effective method for managing postoperative pain and decreasing the need for systemic analgesia. Autogenous bone grafts for rhinoplasty are most useful for grafting of the upper third of the nose and are obtained from the calvarium, the rib, or, less frequently, the iliac crest. Calvarial bone, which is membranous bone, resists resorption and maintains contour more effectively than iliac bone, which is of endochondral origin. Calvarial bone is also associated with less donor site morbidity, although complications of cerebrospinal fluid leakage, sagittal sinus laceration, intracranial injury, and subdural hematoma have been described. Calvarial bone is harvested as a split calvarial bone graft through a hemicoronal incision over the parietal skull. Rib cartilage is much preferred to rib bone grafts. Although autogenous bone grafting is well established in the rhinoplasty literature, we seldom use these donor sites because of susceptibility to fracture, greater difficulty of carving and securing grafts, tendency for a rigid tip or visible graft step off, and the potential for significant donor site morbidity.
Various other autogenous materials are also useful for soft tissue augmentation in rhinoplasty, principally as adjuncts to structural grafting. Examples include costal perichondrium (collected at the time of costochondral graft harvest), temporalis fascia, and fibroadipose tissue from the post auricular region that can be flattened into a thin sheet with an otologic fascia press. Each of these tissues can be harvested with little or no additional donor site morbidity. These grafts may confer significant aesthetic benefit by softening the frameworksoft tissue interface. Most commonly, these tissues are used to camouflage cartilage grafts or to correct minor contour irregularities. In revision rhinoplasty, soft tissue may be used to underlay skin that is thin and atrophic secondary to scarring, contracture, or steroid injection. This soft tissue decreases the risk for graft extrusion, prevents bossae formation, protects the overlying soft tissue skin envelope, and improves the overall quality of the skin envelope. Tragal cartilage or perichondrium may also be used for small grafts.
Homologous Grafts
The most commonly used homografts are irradiated rib for structural grafting and acellularized dermal matrix for soft tissue augmentation. Historically, these grafts, derived from human cadavers, have proved less predictable than autogenous tissue in their ability to resist resorption and warping; however, experience has been mixed. The potential risk for transmission of human pathogens also remains a concern for patients. Nonetheless, these grafting materials are useful in selected patients who are poor candidates for harvest of autogenous tissue or who are unwilling to have an additional donor site. These situations occur only rarely. Costal cartilage homografts are harvested from prescreened cadavers and are subjected to at least 30,000 Gy of radiation to decrease antigenicity. These grafts are associated with low infection and extrusion rates, although soaking in antibiotic solution before use is still recommended. Acellularized dermal matrix has been shown to have significant resorption within the first year, although this tendency for resorption may stabilize there after. Because of this limitation, acellularized dermal matrix is more appropriately used for graft camouflage and smoothing contour under thin skin than for volume augmentation.
Alloplasts
In recent years, alloplasts have become more popular because of their relative ease of use, limitless supply, predesigned or easily adaptable shape, and lack of donor site morbidity. Most alloplasts are polymers, which are long chains of molecular subunits. The more commonly used implants include expanded porous polytetrafluoroethylene (e-PTFE; Gore-Tex), porous high density polyethylene (PHDPE; Medpor), polyester fiber mesh (Mersilene), and silicone, which is used primarily in Asian patients who have thick skin. The biologic response elicited by the host after use of an allograft is influenced by the chemical composition and the physical characteristics of the graft. The implantation of all alloplasts causes an inflammatory response. In the acute phase, neutrophils and macrophages are recruited, and protein material coats the implant. Fibroblasts deposit collagen, and phagocytosis occurs for implant particles smaller than 60 micrometers; particles larger than 20 micrometers cause macrophage death and secondary release of local inflammatory mediators.
The presence and size of pores influence the tendency for fibrovascular ingrowth and the risk for infection. Alloplasts with pores that are greater than approximately 50 micrometers will exhibit tissue ingrowth, with larger pores supporting correspondingly greater ingrowth. PHDPE has large pores that permit soft tissue and limited bony ingrowth. These PHDPE grafts are difficult to remove, but they are also more resistant to infection. In contrast, e-PTFE has smaller pores, making it more readily removable after implantation. Silicone forms a fibrous capsule without ingrowth and carries a persistent risk for extrusion throughout the life of the patient. Not all synthetic agents have withstood the test of time. Polyamide mesh (Supramid), which exhibited excessive degradation and resorption in animal models, is now of historic interest only. Polytetrafluoroethylene (Proplast) demonstrated fragmentation with mechanical stress in temporomandibular joint surgery, leading to its removal from the United States market.
Specific Grafting Techniques
Many grafting techniques have been described for use in primary and revision rhinoplasty. These techniques are categorized by anatomic site in the discussion that follows. Although the descriptions are intended to reflect common uses of particular grafts, many techniques are versatile and can be adapted to suit the particular deformity encountered. Furthermore, this article covers only the more common grafts used in rhinoplasty. Many of these grafts may be placed by either endonasal or external rhinoplasty approaches. The endonasal approach avoids a columellar scar and may reduce postoperative edema; however, in the severely overresected nose, an external rhinoplasty approach should be considered. The external approach allows for improved diagnosis and is most conducive to reconstructing major framework deficiencies, performing precise graft placement, and correcting asymmetries.
Grafts of the Nasal Tip
Columellar struts
The columellar strut provides structural support to the nasal tip and improves tip projection. It has become one of the workhorse grafts in rhinoplasty. As shown in Fig. 2, the graft is placed between the paired intermediate and medial crura, using either an endonasal or open rhinoplasty approach. The need for a strong columellar strut is most evident in noses with short, weak, or flared medial and intermediate crura. For endonasal positioning, an incision may be made in the columella, usually caudal to the medial crura. Alternatively, an incision may be made either through a small vertical incision between the medial crura or through the skin of the nasal vestibule and medial crura on one side. When using an open rhinoplasty approach, the graft is sutured to the medial crura. Care should be taken to avoid unintended distortion of the nasal tip contour or the infratip lobule. The graft must be placed short of the domes to avoid excessive prominence with a ”unidome” configuration. Preserving a small amount of soft tissue over the nasal spine prevents clicking and displacement of the graft with lip movement. For greater stability, the columellar strut may be secured to the nasal spine or premaxilla. Septal or costal cartilage is preferable, although double-layered auricular cartilage will often provide sufficient strength. Using the perpendicular plate of the ethmoid or other bone grafts is also effective but requires perforation before suturing. In the patient who has a dependent caudal septum requiring increased projection, establishing a tongue-ingroove relationship between the medial crura and the nasal septum will achieve stability similar to a columellar strut without the need for graft placement.

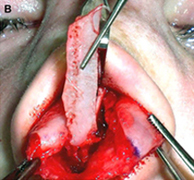
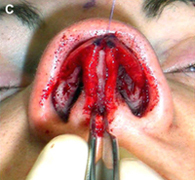
Fig. 2. Columellar strut. The columellar strut, one of the ”workhorse” grafts of structural rhinoplasty, is placed between the paired intermediate and medial crura. (A) Lateral view. (B) Placement of graft. (C) Columellar strut in position.
Onlay tip grafts
These grafts are placed over the alar domes as single or multilayer grafts (Figs. 3 and 4), using either an endonasal or an external approach.
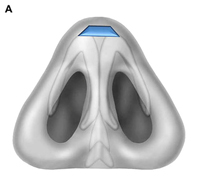
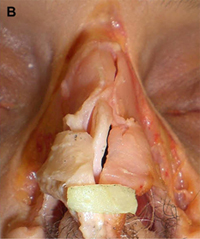

Fig. 3. Tip grafting. (A) Base view, showing beveled edges of graft that minimize visible edges. (B) Peck graft, with its classically rectangular shape. (C) Cap graft. Cephalic volume reduction of the lower lateral cartilage provides donor cartilage that may be used as a cap graft of the nasal tip.
These grafts are used primarily to camouflage irregularities or to achieve subtle increases in tip projection or contour. Beveling or morselization of the edges minimizes the likelihood of visibility or palpability. The Peck graft (see Fig. 3) is a type of onlay tip graft that is made from conchal or septal cartilage. It is classically rectangular and abuts on the domes. The contoured auricular projection graft is a saucer like disc of cartilage taken from the concha cymba or concha cavum and is useful in rhinoplasty on Asian patients. Cap grafts are classically derived from remnant cartilage after cephalic volume reduction of the lower lateral cartilage (see Fig. 3). These cap grafts are small nasal tip grafts used to soften or fill areas of clefting at the nasal tip. They are helpful in improving the contour of the nasal tip in patients who have thin skin. The graft is placed in the space between the tip defining points and the medial crura. The term ”umbrella graft” is used to describe the use of an onlay tip graft in conjunction with a columellar strut; the columellar strut is the umbrella shaft and the tip onlay graft secured to it forms the top of the umbrella (Fig. 5). Placement of tip grafts over the tip defining points will increase tip projection and definition, whereas placement of these grafts at and below the tip defining points will increase projection and add volume to the infratip lobule. Whenever possible, it is desirable to stabilize the grafts within a precise pocket. Securing the grafts with fine sutures, particularly with stacked grafts, also minimizes the risk for graft displacement.
Shield grafts
Shield grafts, sometimes termed Sheen or infralobular grafts, are shield shaped grafts that are positioned over the medial crura, extending from the medial crural footplates to the nasal tip. Examples of these grafts are shown in Fig. 6. Initial enthusiasm for these grafts was considerable because of their usefulness in increasing tip projection, defining the nasal tip, and improving the contour of the infratip region. However, the tendency of these grafts to leave a visible ”tombstone” impression on the overlying skin subsequently led to much more selective usage. These grafts are best reserved for patients who have thick skin, and the edges should be extensively beveled to minimize visibility. Morselization may be beneficial. The extended shield graft, sometimes termed an ”extended columellar strut tip graft”, extends anteriorly beyond the domes to provide added tip projection. In such cases, a small cartilage block placed beneath the graft at the level of the nasal tip may be helpful to increase stability and projection, as shown in Fig. 6. These grafts provide the added benefit of derotation of the overrotated nose. The use of conchal cartilage for this graft improves its pliability and confers a softer contour, thereby decreasing the risk for a visible graft silhouette after resolution of edema.
Other grafts of the nasal tip

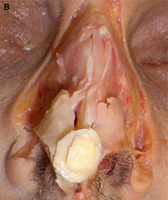
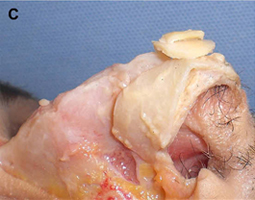
Fig. 4. Multilayer tip grafts. Two or more cartilage grafts, usually secured together with suture, may be stacked to achieve greater projection than is possible with a single graft. (A) Frontal view. (B) Frontal view of tip graft shown in cadaver with soft tissue skin envelope removed. (C) Lateral view.



Fig. 5. Umbrella graft. This graft integrates an onlay tip graft with a columellar strut; the columellar strut is the umbrella shaft and the tip onlay graft is the top of the umbrella. (A) Frontal view. (B) Lateral view. (C) Base view of umbrella graft in anatomic position.
Other, less common, grafts also warrant mention. The anchor graft, so named for its shape, has paired transversely oriented curved wings (Fig. 7). It is carved from auricular cartilage and is used to replace or reinforce the lateral crura, thereby enhancing tip support or projection. The subdomal graft, which is placed transversely as a bar under the domes, is used to correct dome asymmetry. It has found application in the correction of the pinched nasal tip and in stabilizing the vertical and horizontal orientation of the domes. Various autogenous materials are useful in softening the appearance of cartilaginous grafts and in camouflaging subtle irregularities that may become unmasked in the weeks to months after surgery, as the edema resulting from the operation gradually resolves (Fig. 8 ). Fibroadipose tissue or temporalis fascia are readily harvested from the postauricular region, often at the time of conchal cartilage harvest. Use of perichondrium, crushed cartilage, or connective tissue should always be considered when performing rhinoplasty on patients who have thin skin.
Grafts of the Alar Region


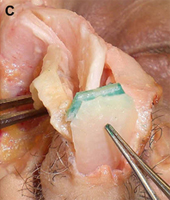
Fig. 6. Shield grafts. Sometimes termed ”Sheen” or ”infralobular” grafts, these shield-shaped grafts are carved in various shapes and then positioned over the medial crura, extending from the medial crural footplates toward the nasal tip. (A) Frontal view, showing examples of various types of shield grafts. (B) Base view of shield graft. Note beveling of edges to avoid a visible ”tombstone” appearance through skin. (C) Extended shield graft with small cartilage block (green) to improve stability and projection.

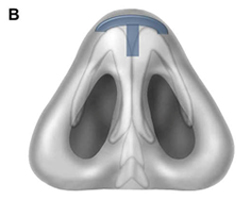
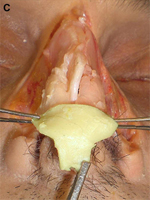
Fig. 7. Anchor graft. This modified infratip shield graft, named for its characteristic shape with curved wings, is used to enhance tip projection, improve alar rim position, and augment the infratip region. (A) Frontal view. (B) Base view. (C) Anchor graft shown in cadaver with soft tissue skin envelope removed.
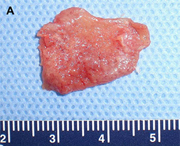


Fig. 8. Autogenous camouflage grafts. These grafts can camouflage subtle contour irregularities and soften the appearance of cartilaginous grafts. They are particularly useful in patients who have thin skin. (A) Perichondrium. (B) Postauricular incision for harvest of conchal cartilage allows access to plentiful fibroadipose tissue. (C) Crushed cartilage
Alar batten grafts
Aesthetic and functional impairment may arise from deformity of the external nasal valve or internal nasal valve, or deepening of the alar nasal groove (Fig. 9). Alar batten grafts, shown in Fig. 10, are placed in a pocket that extends from the piriform aperture to the paramedian position. The exact position of the graft is determined by the site of maximal collapse. Therefore, the graft may extend inferior to the caudal aspect of the lateral crus or even toward the alar rim for correction of an overresected lateral crura or external nasal valve collapse. More cephalad positioning allows for treatment of internal nasal valve collapse. Care must be taken with the grafts to avoid creation of a bulbous appearance or visible prominence. In patients who have thin skin, lateral crural strut grafts (discussed below) may be used to achieve improved airway patency with minimal risk for distortion. Auricular cartilage and septal cartilage are most commonly used, although PHDPE grafts are also available.
When placed through an external rhinoplasty approach, we suture fixate the graft to the surface of the lateral crura in at least two locations to ensure adequate stability. Precise pocket preparation is necessary for endonasal placement. In either approach, we routinely place a 5-0 absorbable suture from the vestibular lining, through the lower lateral cartilage in the hinge area, and through the graft and alar skin. A small cutaneous stab incision is then made adjacent to the projecting needle tip to avoid dimpling, and the suture is brought back through the tissues as a simple stitch and tied intranasally.
Alar rim grafts
Alar rim grafts, sometimes referred to as alar contour grafts, are useful in the prevention or correction of alar retraction (Fig. 11). These grafts also afford the alae sufficient rigidity to resist collapse, as would otherwise occur in cases of cephalic malposition of the lower lateral cartilages. Additional uses include correction of alar flare and treatment of alar contour irregularity. Cartilaginous alar grafts are nonanatomic grafts that are placed in a subcutaneous pocket immediately above the alar rim. They can be placed through an external rhinoplasty approach, a marginal incision, or a small stab incision just inside the alar margin. Alar rim grafts should be placed so that they do not cross the soft tissue triangle, and the leading edge can be softened to avoid bossae formation. When we place these grafts through an external approach, we stabilize them with a 6-0 absorbable suture anteriorly, thereby avoiding migration superiorly. These grafts are typically capable of achieving 1 to 2 mm of inferior displacement of ala. A large alar batten that extends caudally functions as a combined alar batten and alar rim graft.

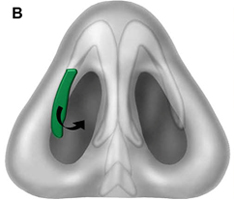
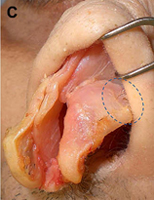
Fig. 9. Sites of nasal collapse. (A) Internal and external nasal valve collapse occurs in the purple region, which spans the lower third of the nose and caudal aspect of the nasal midvault, including the hinge area. Alar batten grafts can be placed anywhere in this region. The midvault (blue region) is classically stented with spreader grafts. Nasal bones (green) denote upper third of nose. (B) Recurvature of the lower lateral crura (green) narrows the nasal airway and can be corrected with cartilaginous grafting. (C) Collapse at hinge area on cadaveric specimen is denoted by the broken line ellipse.


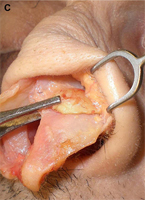
Fig. 10. Alar batten grafts. These grafts extend from the piriform aperture to the paramedian position and are positioned at the site of maximal collapse. (A) Frontal view showing standard position of alar batten grafts in blue. Purple indicates the larger range of possible placement for these grafts, depending on the site of collapse. (B) Three-quarter view showing a large alar batten graft carved from auricular conchal cartilage. The graft convexity will promote nasal airway patency. (C) Graft in position.


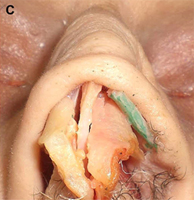
Fig. 11. Alar rim grafts. Also referred to as alar contour grafts, these grafts are used to correct alar retraction and to provide support to the external nasal valve. (A) Frontal view. (B) Lateral view. (C) Alar rim graft in anatomic position.
Composite grafts
In cases of severe alar retraction, where a rim graft will not achieve adequate correction, a composite graft is necessary (Fig. 12). Composite grafts typically consist of skin, cartilage, and the intervening perichondrium and connective tissue elements. These grafts may be harvested from various locations, including the concha cymba, concha cavum, or auricular root. Usually, the cartilaginous portion of the graft is larger than the overlying skin to maximize the structural augmentation. These grafts are also beneficial in the treatment of vestibular stenosis.
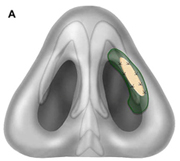
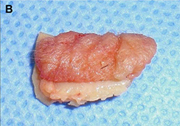

Fig.12. Composite grafts. These grafts are useful in the treatment of vestibular stenosis and correction of severe alar retraction not amenable to rim grafting. (A) Base view shows composite graft in nasal vestibule. Note that the structural cartilaginous component of the graft (green) is larger than the overlying skin component (stippled pink). (B) Composite graft. (C) Auricular cartilage showing common sites of graft harvest, including concha cymba (red), concha cavum (blue), and auricular root (green).
Lateral crural strut graft
The lateral crural strut graft, shown in Fig. 13, is well suited to the thin skinned patient who has a moderate degree of alar collapse and in whom an unfavorable aesthetic result would be expected with alar batten grafting. Lateral crural strut grafts allow for correction of alar rim collapse, deformed lateral crura, and mild alar retraction. These grafts, like alar batten grafts, are effective for straightening the lateral crus, especially when recurvature of the lower lateral crura is present. These grafts are also useful in providing support to the nasal tip when cephalic malposition is present and the alae must be repositioned. These grafts require dissection of the vestibular skin from the undersurface of the lower lateral cartilage and are placed between the lateral crus and the vestibular skin. The lateral aspect of the rim graft is usually positioned superficial to the piriform aperture and caudal to the alar groove. Although extremely useful, these grafts are more technically difficult than batten grafts. They also tend to protrude slightly into the nasal airway and impart less structural rigidity than alar batten grafts.
Other grafts of the alar region
Several other, less common, alar grafts have also been described. The lateral crural spanning graft, also referred to as an alar spreader graft, is a transverse graft that spans the intercrural space (Fig. 14).This graft allows for correction or prevention of an overly narrowed or pinched nasal tip. It is secured to both lateral crura for stabilization and must be beveled to avoid being discernable postoperatively. These grafts may make the tip more bulbous if not carefully contoured. Lateral crural turnover grafts are used to create thicker and stronger lateral crura. Longitudinal scoring or partial thickness incision along the undersurface of the lateral crura is followed by suturing of the cephalic portion of the lateral crura to its caudal remnant.41 The lateral crural onlay graft is used to strengthen and shape alae that are weakened or have irregular contour. The grafts are placed over the lateral crus to improve external nasal valve function. This graft has some similarity to the alar batten graft, although it more closely mirrors alar cartilage anatomy. Care must be taken to bevel these grafts so as to avoid a ”step off” deformity.
Grafts of the Nasal Dorsum and Midvault
Spreader grafts (and extended spreader grafts) Spreader grafts, shown in Fig. 15, are longitudinally oriented grafts, usually paired, that are secured deep to the mucoperichondrium between the nasal septum and upper lateral cartilages.


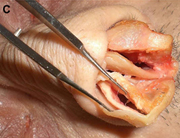
Fig. 13. Lateral crural strut grafts. These inconspicuous grafts are placed deep to the alar cartilage and allow for correction of moderate alar collapse, lower lateral cartilage recurvature, and mild alar retraction. (A) Vestibular lining is dissected away from the undersurface of the lower lateral cartilage, creating a pocket for graft placement. (B) Placement of graft. (C) Lateral crural strut graft in anatomic position.

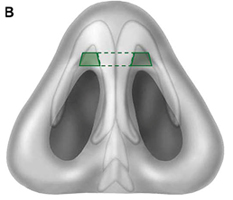

Fig. 14. Lateral crural spanning graft. Also referred to as an alar spreader graft, this graft allows for correction of an overly narrowed or pinched nasal tip. (A) Frontal view. (B) Base view. (C) Graft shown in anatomic position.
These grafts are among the most commonly used and versatile grafts in both primary and revision rhinoplasty. They are frequently used to reconstruct an open roof deformity and to smooth the brow-tip aesthetic line. Spreader grafts prevent or correct midvault collapse by stenting open the internal nasal valve, thereby avoiding medial displacement of the upper lateral cartilages. Occasionally, grafts with asymmetric width are helpful in managing pre-existing midvault irregularities. We usually place these grafts through an external approach to facilitate suture fixation after the upper lateral cartilages and septum are separated. We seldom place spreader grafts beneath intact lower lateral cartilages because this method produces less reliable outcomes. Several adaptations to the spreader grafts have been described. The term ”pistol grafts” refers to spreader grafts that extend above the dorsal septum to augment the dorsum. When performing this maneuver, it is important to appropriately camouflage the irregularity that is produced. When spreader grafts project caudally to lengthen the nose or increase tip projection, they are referred to as extended spreader grafts or septal extension grafts. The caudal ends of the grafts are sutured to the medial surfaces of the intermediate crura of the lower lateral cartilages, thereby providing tip derotation. The dynamic adjustable rotational tip (DART) grafts are long spreader grafts used to correct tip deprojection and overrotation in patients who have overly resected, weakened cartilage frameworks.44 Spreader grafts may also extend cephalically to slightly widen the bony nasal pyramid, although widening at this site is only occasionally indicated.


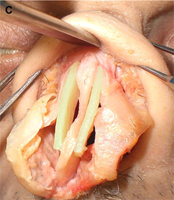
Fig. 15. Spreader grafts. These grafts, which have become the workhorse for midvault reconstruction, are used to correct or prevent collapse of the middle third of the nose, to reconstruct open roof deformity, and to smooth the brow-tip aesthetic line. (A) This axial section through the midvault demonstrates how spreader grafts can expand the nasal airway. (B) Frontal view. (C) Spreader grafts in anatomic position.
Septal extension grafts and septal replacement grafts
Septal extension grafts include various grafts that are used to enhance nasal tip dynamics by building stable framework onto the existing septal scaffold. The size and position of septal extension grafts are varied to influence projection, to derotate the tip, or to fill out the columella labial angle, thereby suggesting tip rotation. Some septal extension grafts are actually long spreader grafts that span from the nasal septum, beyond the anterior septal angle, and into the interdomal region (Fig. 16). A second type of septal extension graft involves cartilage grafts that run diagonally from the septal angle to the tip–lobule complex. The third type of graft, sometimes termed a ”caudal septal extension graft”, is a direct extension from the caudal septum that can control the projection, rotation, and strength of the tip (Fig. 17). This graft confers considerable strength and stability because of its rigid foundation. The medial crura can be repositioned along this augmented septum, and lateral crural steal may be used to optimize tip projection. In cases in which a caudal septum is weak or missing, resulting in alar columellar disproportion, a septal extension graft or caudal septal replacement graft (Fig. 18) will improve tip support and correct columellar retraction.



Fig.16. DART grafts stabilized with columellar strut. These elongated spreader grafts extend into the dome as septal extension grafts and can increase projection and derotate the tip. Stability is optimized when they are integrated with a columellar strut, as depicted in these figures. (A) Frontal view. (B) Lateral view. (C) Grafts in anatomic position.



Fig.17. Caudal septal extension graft. This graft extends directly from the caudal septum to control the projection, rotation, and strength of the nasal tip. (A) Lateral view, showing columellar strut (green) secured to nasal septum (red). (B) Placement of graft. (C) Graft in anatomic position.


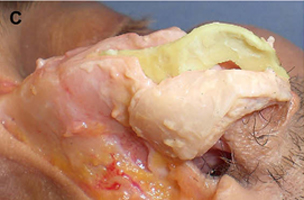
Fig. 18. Caudal septal replacement graft. This graft is useful when the caudal septum is weak, deformed, or absent. (A) Lateral view. (B) Frontal view. (C) Graft in anatomic position.
Dorsal onlay graft
The dorsal onlay graft, shown in Fig. 19, is used to correct minor and major deformities of the nasal dorsum. Commonly, we design these grafts to span the entire length of the nasal dorsum, from the radix to the septal angle, to minimize the risk for palpable irregularities. Smaller refinement grafts may be used as beveled or crushed grafts to address contour irregularities or asymmetries. Although septal or conchal cartilage is usually sufficient for refinement of the nasal dorsum, costal cartilage is indicated in those cases where major augmentation is required. Examples include severe saddle nose deformity, traumatic compressive fractures, or other major structural deficits. Alternatives are e-PTFE, PHDPE, and silicone (in patients who have thick skin), although autogenous material is preferred. If e-PTFE is used, we avoid dissection that communicates to dorsal and septal surgical sites because we believe that doing so increases the risk for alloplast infection. We routinely harvest a ”floater” rib, which is straighter and less prone to warping than the sixth or seventh rib. This floater rib is harvested as half bone and half cartilage, thereby mirroring the natural osseocartilaginous anatomy of the nasal dorsum. The bony portion of the graft is positioned cephalically, and the undersurface is carved in a gently curving concave contour to ensure that the graft will be seated firmly and to expose the cancellous trabecular bone. Before securing the graft, the surgeon then rasps down the bony foundation where the graft will sit until punctuate bleeding is encountered. The contact of raw bone to raw bone thus achieved promotes effective osseointegration of the cantilevered graft to the underlying bony foundation. The dorsal onlay graft obviates the need for spreader grafts because the upper lateral cartilages are sutured to the lateral cartilaginous aspects of the graft. The graft is then rigidly fixated with a percutaneous Kirschner wire (K-wire) that further promotes rigid fixation and minimizes the risk for warping. The K-wire is easily removed in the office in 3 weeks.


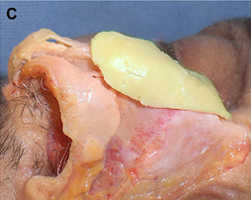
Fig. 19. Dorsal onlay graft. Septal and auricular cartilage are useful for improving the contour of the nasal dorsum, whereas costal cartilage is indicated in cases where major augmentation is required, as in severe saddle nose deformity. (A) Frontal view. (B) Lateral view. (C) Graft shown in cadaver with soft tissue skin envelope removed.
Rarely, it is necessary to articulate the dorsal graft and a columellar strut. This approach is most useful when a profound loss of structural support in the lower third of the nose occurs. For example, in patients who have significant saddle deformity, the lower third of the nose is usually poorly supported, and a strong cartilaginous columellar strut is required, along with an integrated cartilaginous premaxillary graft. The columellar strut and premaxillary graft are placed through an open rhinoplasty approach with dissection between the medial crura. The premaxillary graft is fixated with a percutaneous K-wire.
Skoog technique modification
In patients who have short nasal bones and long upper lateral cartilages, a modification of the Skoog technique for dorsal reduction may be advantageous (Fig. 20). In this procedure, the osseocartilaginous dorsal convexity is removed as a unit, the underlying nasal dorsum is reduced, and the osseocartilaginous unit is then sculpted by shaving off the residual septal remnant on the undersurface and replaced in it is original anatomic location. The upper lateral cartilages are subsequently secured to this anatomic osseocartilaginous graft with suture fixation. This approach is attractive from aesthetic and functional aspects because it accomplishes dorsal reduction, correction of the open roof deformity, preservation of the middle vault, and restoration of the natural contouring of the nasal dorsum while obviating the need for osteotomies.



Fig. 20. Modified Skoog procedure. In patients who have short nasal bones and long upper lateral cartilages, the osseocartilaginous dorsal convexity is removed and sculpted for use as a dorsal onlay graft after appropriate reduction of the underlying nasal dorsum. (A) Dashed line denotes osseocartilaginous convexity to be removed with scalpel and Rubin osteotome. (B) Cadaveric demonstration of regions to be sculpted into onlay graft. (C) Sculpted onlay graft showing short nasal bones and long cartilaginous component.
Radix graft
Radix grafts, shown in Fig. 21, are used to reposition the radix in a more cephalic and anterior position. This maneuver provides the perception of lengthening the nose and can also be used to augment an inadequate nasofrontal angle. Precise subperiosteal pocket preparation minimizes the risk for graft displacement. The grafts may be single or layered, and beveling or crushing of the sides of the grafts will decrease perceptibility.

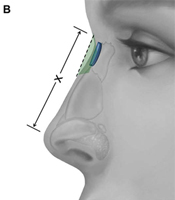
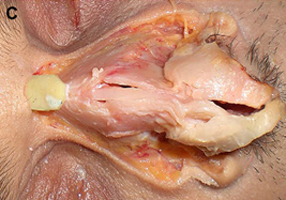
Fig. 21. Radix graft. This graft allows for augmentation of the nasofrontal angle and creates the perception of nasal lengthening by repositioning the radix. (A) Frontal view, with peripheral aspect of cartilaginous graft crushed (crosshatches) to minimize visibility. (B) Lateral view. Green shading and broken line indicate radix being repositioned in a more cephalic and anterior position, thereby increasing nasal length, denoted by ”X.” (C) Graft shown in cadaver with soft tissue skin envelope removed.
Deficiency of the radix is easily overlooked and may prompt excessive resection of the nasal dorsum if the dorsum is brought down to the level of the radix. Significant iatrogenic deformity can result from this error in judgment. Thoughtful application of this simple, yet powerful, grafting technique can yield satisfying results. The aesthetic perception of nasal lengthening achieved with this graft, although limited, is far more predictable than the lengthening achieved by stretching the soft tissue skin envelope and increasing projection. Furthermore, the radix graft does not pose the risk for introducing asymmetry or other deformity to the lower third of the nose.
Lateral nasal wall grafts
Lateral nasal wall grafts, also referred to as dorsal sidewall onlay grafts, are grafts of variable size that are used to correct focal depression or contour irregularity along the lateral nose. The grafts are positioned along the lateral aspect of the nose in the area of asymmetry and tend to be most useful in the midvault region. The grafts may be crushed or rigid, although rigid grafts are more likely to be discernible when placed over the bony pyramid of the upper third of the nose. When a cosmetic deformity of the midvault is associated with nasal airway obstruction, either spreader grafts or another grafting technique that simultaneously addresses the functional problem should be used.
Columellar plumping grafts
Columellar plumping grafts, shown in Fig. 22, consist of diced or morselized cartilage that is placed at the posterior aspect of the columella. Placing graft material in the region between the nasal spine and medial crural footplates results in widening of the columellar labial angle. This graft thus creates an appearance of nasal tip rotation.



Fig. 22. Columellar plumping grafts. Diced or morselized cartilage is placed between the nasal spine and footplates of the medial crura to widen the columellar-labial angle. This technique creates the illusion of tip rotation. (A) Frontal view. (B) Lateral view. Green shading and broken line indicated widening of the columellar-labial angle, X . (C) The plumping grafts, shown in figure, are placed subcutaneously.
Premaxillary grafting
The premaxillary graft is used to augment an underdeveloped or retrusive premaxilla. It involves grafting of the caudal aspect of the piriform aperture. These grafts may be difficult to carve and, depending on the underlying anatomy, may require substantial volume. In rhinoplasty in Asians, silicone implants are often used and thought to be better tolerated because of the thicker skin in this ethnic population. Costal cartilage is another option well suited to this location, particularly if the use of costal cartilage for another part of the reconstruction is already indicated.
Alar base grafts
Alar base grafts are used along the lateral piriform aperture to augment a posteriorly displaced interface of the lip and ala. The alar base composite graft is particularly useful in reconstruction of the cleft lip nasal deformity. This deformity exemplifies how the lack of a stable platform in the premaxilla precludes a normal relationship between the lip and nose. In cases of significant bony deficiency of the premaxilla, a corticocancellous bone graft may be necessary to reconstruct the underlying deformity.
Summary
The development of sophisticated grafting techniques has played an integral role in achieving durable surgical outcomes in rhinoplasty. The loss of structural integrity often encountered after reductive rhinoplasty illustrates the importance of preservation of framework. The structural approach to rhinoplasty uses grafts to maintain and augment nasal support mechanisms and in doing so, enables the nasal skeleton to resist contractile forces of healing that would otherwise compromise aesthetic and functional results.
Acknowledgments
The authors wish to thank Eric Dobratz, MD, for his assistance with the laboratory dissections used for selected figures in this publication.
References
- Adamson PA. Grafts in rhinoplasty: autogenous grafts are superior to alloplastic. Arch Otolaryngol Head Neck Surg 2000;126(4):561–2.
- Toriumi DM. Autogenous grafts are worth the extra time. Arch Otolaryngol Head Neck Surg 2000;126(4):562–4.
- Quatela VC, Jacono AA. Structural grafting in rhinoplasty. Facial Plast Surg 2002;18(4):223–32.
- Toriumi DM, Patel AB, Derosa J. Correcting the short nose in revision rhinoplasty. Facial Plast Surg Clin North Am 2006;14(4):343–55.
- Whitaker EG, Johnson CM Jr. The evolution of open structure rhinoplasty. Arch Facial Plast Surg 2003;
5(4):291–300. - Biesman B. Soft tissue augmentation using Restylane. Facial Plast Surg 2004;20(2):171–7.
- Gunter JP, Rohrich RJ. Augmentation rhinoplasty: dorsal onlay grafting using shaped autogenous septal cartilage. Plast Reconstr Surg 1990;86(1):39–45.
- Ortiz-Monasterio F, Olmedo A, Oscoy LO. The use of cartilage grafts in primary aesthetic rhinoplasty. Plast Reconstr Surg 1981;67(5):597–605.
- Tardy ME Jr, Denneny J III, Fritsch MH. The versatile cartilage autograft in reconstruction of the nose and face. Laryngoscope 1985;95(5):523–33.
- Cakmak O, Bircan S, Buyuklu F, et al. Viability of crushed and diced cartilage grafts: a study in rabbits. Arch Facial Plast Surg 2005;7(1):21–6.
- Smith JD, Abramson M. Membranous vs endochondrial bone autografts. Arch Otolaryngol 1974;99(3):203–5.
- Frodel JL Jr, Marentette LJ, Quatela VC, et al. Calvarial bone graft harvest. Techniques, considerations, and morbidity. Arch Otolaryngol Head Neck Surg
1993;119(1):17–23. - Romo T III, Jablonski RD. Nasal reconstruction using split calvarial grafts. Otolaryngol Head Neck Surg
1992;107(5):622–30. - Guerrerosantos J. Nose and paranasal augmentation: autogenous, fascia, and cartilage. Clin Plast Surg 1991;18(1):65–86.
- Adams WP Jr, Rohrich RJ, Gunter JP, et al. The rate of warping in irradiated and nonirradiated homograft rib cartilage: a controlled comparison and clinical implications. Plast Reconstr Surg 1999;103(1):265–70.
- Dingman RO, Grabb WC. Costal cartilage homografts preserved by irradiation. Plast Reconstr Surg Transplant Bull 1961;28:562–7.
- Song HM, Lee BJ, Jang YJ. Processed costal cartilage homograft in rhinoplasty: the Asian Medical Center experience. Arch Otolaryngol Head Neck
Surg 2008;134(5):485–9. - Strauch B, Wallach SG. Reconstruction with irradiated homograft costal cartilage. Plast Reconstr Surg 2003;111(7):2405–11.
- Gryskiewicz JM, Rohrich RJ, Reagan BJ. The use of AlloDerm for the correction of nasal contour deformities. Plast Reconstr Surg 2001;107(2):
561–70. - 20. Sclafani AP, Romo T III, Jacono AA, et al. Evaluation of acellular dermal graft (AlloDerm) sheet for soft tissue augmentation: a 1-year follow-up of clinical observations and histological findings. Arch Facial Plast Surg 2001;3(2):101–3.
- Conrad K, Torgerson CS, Gillman GS. Applications of
GORE-TEX implants in rhinoplasty reexamined after
17 years. Arch Facial Plast Surg 2008;10(4):224–31. - Turegun M, Acarturk TO, Ozturk S, et al. Aesthetic and functional restoration using dorsal saddle shaped Medpor implant in secondary rhinoplasty. Ann Plast Surg 2008;60(6):600–3.
- Colton JJ, Beekhuis GJ. Use of mersilene mesh in nasal augmentation. Facial Plast Surg 1992;8(3):149–56.
- Romo T III, Kwak ES. Nasal grafts and implants in revision rhinoplasty. Facial Plast Surg Clin North Am 2006;14(4):373–87.
- Sclafani AP, Romo T III. Biology and chemistry of facial implants. Facial Plast Surg 2000;16(1):3–6.
- Sclafani AP, Thomas JR, Cox AJ, et al. Clinical and histologic response of subcutaneous expanded polytetrafluoroethylene (Gore-Tex) and porous highdensity polyethylene (Medpor) implants to acute and early infection. Arch Otolaryngol Head Neck Surg 1997;123(3):328–36.
- Anderson JR. A new approach to rhinoplasty. Trans Am
Acad Ophthalmol Otolaryngol 1966;70(2):183–92. - Peck GC. The onlay graft for nasal tip projection.
Plast Reconstr Surg 1983;71(1):27–39. - Porter JP, Tardy ME Jr, Cheng J. The contoured auricular projection graft for nasal tip projection. Arch Facial Plast Surg 1999;1(4):312–5.
- Peck GC Jr, Michelson L, Segal J, et al. An 18-year experience with the umbrella graft in rhinoplasty. Plast Reconstr Surg 1998;102(6):2158–65.
- Sheen JH. Achieving more nasal tip projection by the use of a small autogenous vomer or septal cartilage graft. A preliminary report. Plast Reconstr Surg
1975;56(1):35–40. - Pastorek NJ, Bustillo A, Murphy MR, et al. The extended columellar strut-tip graft. Arch Facial Plast Surg 2005;7(3):176–84.
- Chang CW, Davis RE. The anchor graft: a novel technique in rhinoplasty. Arch Facial Plast Surg
2008;10(1):50–5. - 34. Juri J, Juri C, Grilli DA, et al. Correction of the secondary nasal tip and of alar and/or columellar collapse. Plast Reconstr Surg 1988;82(1):160–5.
- Guyuron B, Poggi JT, Michelow BJ. The subdomal graft. Plast Reconstr Surg 2004;113(3):1037–40.
- Toriumi DM, Josen J, Weinberger M, et al. Use of alar batten grafts for correction of nasal valve collapse. Arch Otolaryngol Head Neck Surg 1997;
123(8):802–8. - Rohrich RJ, Raniere J Jr, Ha RY. The alar contour graft: correction and prevention of alar rim deformities in rhinoplasty. Plast Reconstr Surg 2002;109(7):2495–505.
- Constantian MB. Indications and use of composite grafts in 100 consecutive secondary and tertiary rhinoplasty patients: introduction of the axial orientation. Plast Reconstr Surg 2002;110(4):1116–33.
- Gunter JP, Friedman RM. Lateral crural strut graft: technique and clinical applications in rhinoplasty. Plast Reconstr Surg 1997;99(4):943–52.
- Gunter JP, Rohrich RJ. Correction of the pinched nasal tip with alar spreader grafts. Plast Reconstr Surg
1992;90(5):821–9. - McCollough EG, Fedok FG. The lateral crural turnover graft: correction of the concave lateral crus. Laryngoscope 1993;103(4 Pt 1):463–9.
- Sheen JH, Sheen JH. Spreader graft: a method of reconstructing the roof of the middle nasal vault following rhinoplasty. Plast Reconstr Surg 1984;73(2):230–9.
- Palacin JM, Bravo FG, Zeky R, et al. Controlling nasal length with extended spreader grafts: a reliable technique in primary rhinoplasty. Aesthetic Plast Surg 2007;31(6):645–50.
- Dyer WK, Yune ME. Structural grafting in rhinoplasty.
Facial Plast Surg 1997;13(4):269–77. - Byrd HS, Andochick S, Copit S, et al. Septal extension grafts: a method of controlling tip projection shape. Plast Reconstr Surg 1997;100(4):999–1010.
- Ha RY, Byrd HS. Septal extension grafts revisited: 6-year experience in controlling nasal tip projection and shape. Plast Reconstr Surg 2003;112(7):1929–35.
- Kridel RW, Chiu RJ. The management of alar columellar disproportion in revision rhinoplasty. Facial Plast Surg Clin North Am 2006;14(4):313–29.
- Gunter JP, Clark CP, Friedman RM. Internal stabilization of autogenous rib cartilage grafts in rhinoplasty: a barrier to cartilage warping. Plast Reconstr Surg
1997;100(1):161–9. - Hall JA, Peters MD, Hilger PA. Modification of the Skoog dorsal reduction for preservation of the middle nasal vault. Arch Facial Plast Surg 2004;6(2):
105–10. - Becker DG, Pastorek NJ. The radix graft in cosmetic rhinoplasty. Arch Facial Plast Surg 2001;3(2):115–9.
- Constantian MB. An algorithm for correcting the asymmetrical nose. Plast Reconstr Surg 1989;
83(5):801–11. - Gunter JP, Landecker A, Cochran CS. Frequently used grafts in rhinoplasty: nomenclature and analysis. Plast Reconstr Surg 2006;118(1):
14e–29e. - Deva AK, Merten S, Chang L. Silicone in nasal augmentation rhinoplasty: a decade of clinical experience. Plast Reconstr Surg 1998;102(4):
1230–7. - Lam SM, Kim YK. Augmentation rhinoplasty of the Asian nose with the ‘‘bird’’ silicone implant. Ann Plast Surg 2003;51(3):249–56.
- Pessa JE, Peterson ML, Thompson JW, et al. Pyriform augmentation as an ancillary procedure in facial rejuvenation surgery. Plast Reconstr Surg
1999;103(2):683–6.
©2012 Hilger Facial Plastic Surgery