
Three-dimensional imaging technology has only recently been described in the literature as a means to plan and better understand tissue expansion. This application is a logical use of the technology as the volume changes achieved with tissue expansion are controlled and often dramatic. This article reviews some of the phenomena associated with tissue expansion that are amenable to study with 3-dimensional imaging and reviews selected cases from the literature where the technology has been used to answer clinical questions and plan procedures. The future directions and limitations of the use of this technology in the head and neck will also be described.
of a tissue expander.
TISSUE EXPANSION
Tissue expansion in a form near its modern evolution was first described as a means of head and neck reconstruction in 1957, and it has been proven a safe and effective means of reconstructing many defects in the head and neck. Although expanded tissue undergoes histologic changes, it provides a better color and texture match for many areas of the head and neck than tissue obtained from distant donor sites. Important changes related to tissue expansion include decreased density of hair follicles, increased vascularity of the tissue, and the formation of a fibrous capsule around the expander.
IMPLANT SELECTION
Various tissue expanders are available commercially. The choice of implant is dependent upon the surgeon’s assessment of the defect to be reconstructed. Rectangular implants provide the greatest increase in surface area for the volume added, and oval implants have been shown to give a greater increase in surface area with a lower amount of pressure as compared with round implants. A greater surface area of tissue is obtained from a single oval tissue expander than 2 spherical expanders with a combined volume equal to the oval expander; however, multiple expanders are frequently used in the head and neck because of the complex nature of the anatomy. Overfilling expanders is a safe practice but increases the risk of leak at the injection port.
of tissue expansion.
An accurate assessment of the size of the defect and the amount of skin required to reconstruct the defect is critical to implant selection. This is often based upon 2-dimensional measurements of the defect and adjacent skin. Specifically within the head and neck, linear measurements between points of static bony anatomy (ie, the nasion, angle of mandible, and midpoint of the clavicle) on the side of the defect may be compared with the contralateral normal side in determining the amount of skin required for a given reconstruction. Two-dimensional measurements of complex 3-dimensional defects can be misleading and often underestimate the surface area that will be required to fill a given defect.
POSTERIOR EXPANSION VOLUME AND BONY REMODELING
Tissue expanders can cause significant changes to the tissues underlying the implant that cannot be appreciated while the implant is in place. This phenomenon has been described as posterior expansion volume by Tepper and colleagues as it relates to breast reconstruction. The expander remodels the chest wall; thus some of the volume injected into the expander does not contribute to an increased surface area of skin available for the reconstruction. In this situation, there is a discrepancy between the volume change measured and the volume injected. This phenomenon is seen in the head and neck as well; expanders cause bony remodeling of the calvarium, with bone resorption in the center of the implant and reactive bone formation at the periphery.
CONTRACTION
Once a tissue expander is removed, significant contraction of the expanded tissue is noted in the ensuing weeks and months. Some surgeons will remove all or part of the capsule around the expander, with the thought that the capsule with its increased density of fibroblasts is contributing to this phenomenon. Three-dimensional imaging has proven to be useful in analyzing contraction; a 20% decrease in expanded volume was noted over the 12 months subsequent to reconstruction of a patient with hemifacial microsomia using
3-dimensional photogrammetry.
THREE-DIMENSIONAL ANALYSIS
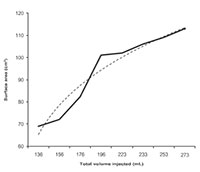
total volume injected increases.
Several means of obtaining 3-dimensional surface images are presently available and are discussed more extensively elsewhere in this issue. Computed tomography (CT)-assisted 3-dimensional imaging generates a 3-dimensional surface image by superimposing photographs onto the surface generated by a CT scan, which is time-consuming and requires radiation exposure. Three-dimensional laser scanners have been in use for some time and use a beam or stripe of laser light to capture multiple data points in space and generate a 3-dimensional image. Scanners are becoming faster and more portable. Stereophotogrammetry uses two or more cameras of a known focal length at different angles to the subject. The computer is able to generate a 3-dimensional rendering of the subject to within a millimeter. The Canfield VECTRA M3 3-D (Canfield Imaging Systems, A Division of Canfield Scientific Inc, Fairfield, ND, USA) camera and accompanying Mirror software were used to analyze data for the case presented in this article.
the bony deficiency, and then serial 3-dimensional photographs were taken, showing that the majority of contraction occurred over the first 3 months. However, over the course of a year, 20% of the total volume gained by expansion was lost. This report was the first in using 3-dimensional photogrammetry to analyze tissue expanders in the head and neck.
THREE-DIMENSIONAL ANALYSIS OF TISSUE EXPANDERS

difference between baseline and
follow-up images showing the total amount
of change in volume over the course of expansion.
Green areas show no change in volume,
and red is 20 mm of expansion.

forehead flap. Costal cartilage was used
for structural support, and turn-in flaps
were used for internal lining inferiorl
Reconstructive surgeons have begun to adopt 3-dimensional surface analysis of tissue expansion over the past decade. Initial reports analyzing cleft patients11 were among the first in using 3-dimensional facial imaging to understand a specific clinical entity and demonstrated the promise that this modality holds for improved understanding of complex facial structures.
Tissue expansion is a logical use for 3-dimensional imaging in that it allows surgeons to follow serial injections of a known volume and observe the effects on surface area over time.
Ying and colleagues first described the use of 3-dimensional analysis of tissue expansion using a laser scanner in a burn patient. Images were taken preoperatively to compare the normal side with the side to be reconstructed, and the difference in surface area was calculated to determine the area of expanded tissue that would be necessary for the repair. This calculation agreed closely with the actual measured size of the cheek defect. Subsequent imaging was performed on postoperative day 12 showing a 44% reduction in the surface area of the flap.
Tepper and colleauges described the use of 3-dimensional analysis of tissue expanders in 12 patients undergoing unilateral breast reconstruction. In the course of their study they used a 3-dimensional laser scanner to analyze patients before mastectomy, during tissue expansion, and postoperatively. The images were used to guide expansion volume, implant selection, and contralateral augmentation or reduction procedures. Overall they found improved breast symmetry when comparing pre and post-reconstructive photographs. They also noted a discrepancy between injected and observed volume, which they attributed to remodeling of the chest wall and termed posterior expansion volume.
Jayaratne and colleagues described the use of 3-dimensional photogrammetry to determine the volume needed in the reconstruction of a patient with hemifacial microsomia by measuring the difference in volume between the 2 sides to be 16 cm3. A tissue expander was placed over the mandible, and serial expansions were performed until the expander had increased the volume to twice the required volume to allow for contraction. The expander was removed; a scapula free flap was used to correct the bony deficiency, and then serial 3-dimensional photographs were taken, showing that the majority of contraction occurred over the first 3 months. However, over the course of a year, 20% of the total volume gained by expansion was lost. This report was the first in using 3-dimensional photogrammetry to analyze tissue expanders in the head and neck.
Case Presentation
the concavity over the right frontal bone
where the expander caused significant expansion.
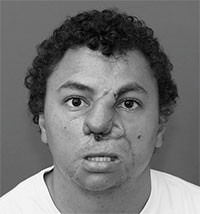
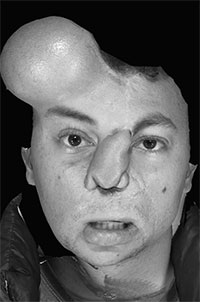
The Canfield VECTRA 3-D camera (Canfield Imaging Systems, A Division of Canfield Scientific Inc, Fairfield, ND, USA) was used to take photos during and after expansion in a patient undergoing an expanded paramedian forehead flap for reconstruction of a post-traumatic nasal defect. This case highlights some of the important uses, limitations, and questions that can be answered using this technology. The patient was a young male who sustained severe facial injuries including a total nasal avulsion with soft tissue loss involving the upper lip. He had undergone multiple reconstructive procedures including a prior nasal reconstruction with a paramedian forehead flap. This reconstruction was complicated by a postoperative infection that caused loss of the structural grafts and partial loss of the paramedian forehead flap (Fig. 1). Due to the scarring from the prior procedure and the large quantity of tissue required for coverage, reconstruction using an expanded paramedian forehead flap was planned. A tissue expander was placed, and serial expansion was performed twice weekly in the clinic with 10 cc of saline until a sufficient amount of nonhairbearing skin was available for the reconstruction (Fig. 2). Due to the fact that half of the expander was buried deep to the scalp, a precise volumetric analysis of the tissue expansion was not possible. The Canfield VECTRA 3D camera and software were used to obtain photographs during expansion and after the nasal reconstruction. The total surface area of skin anterior to the hairline on the expanded side was 113 cm2 versus 38 cm2 on the nonexpanded side. As the expander was partially buried under the scalp, an accurate measure of the volume before and after expansion was not possible. The surface area increased with expansion more rapidly at first and slowed as the total volume of the expander increased (Fig. 3). Volume changes were demonstrated by coregistering images using fixed points on the photographs (ie, medial and lateral canthi, the apex of the previous paramedian forehead flap, and a nevus on the left cheek).

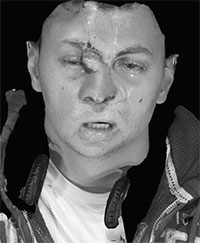
Accurate coregistration was confirmed by creating a color map comparing the volumetric differences between the 2 images as seen in Fig. 4. After expansion was completed, the patient underwent division and inset of his previous forehead flap pedicle; the skin from the previous forehead flap was used as turn-in flaps to create an internal lining inferiorly. Costal cartilage was used to construct dorsal and alar struts as described by Weng and colleagues, and the entire outer cover was reconstructed using expanded forehead skin (Fig. 5). The flap was raised over the expander, and the capsule was excised. Significant bony remodeling of the calvarium was noted with a ridge of reactive bone at the margins of the expander and a depression at the center. After raising and rotating the flap, the forehead was closed primarily with minimal distortion of the hairline. The patient returned to the clinic 2 weeks later for a postoperative visit. His incisions were well healed; there was minimal distortion of his hairline follow-up imaging, continuing to heal well. His nasal projection was improved by 8 mm, yielding a much-improved profile (Fig. 7).
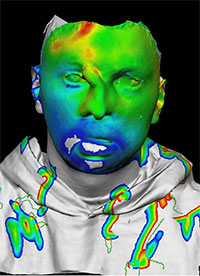
green indicates no volume change.
Note the change in volume over the lower
third of the face; this is an artifact
created by the patient having his jaw slightly
open in 1 photo and not the other.
The volume changes in the upper third
of the face reflect an improvement in
postoperative edema.
Analysis of the 2 and 10 week postoperative views showed a 5 mm difference in the projection of the bony rim around the expander, and a 5 mm decrease in the size of the vascular pedicle, consistent with the observed decrease in soft tissue edema. Overall, the volume of the bony defect in the forehead decreased by 7.5 cm3, consistent with decreased edema but also potentially with some bony remodeling, as the contour of the defect from the tissue expander was visibly improved ( Fig. 8 ). The surface area of the defect decreased from 61.9 cm2 to 54.9 cm2. The projection of the nasal tip was reduced by less than 1 mm. The surface area of the paramedian forehead flap decreased from 24.6 cm2 to 22.2 cm2, contraction of 9.8%.
FUTURE DIRECTIONS
Application of 3-dimensional technology to tissue expanders is in its infancy. 3-dimensional imaging has the potential to help reconstructive surgeons improve surgical planning710 by allowing the precise measurement of surface area and volume. Morphing software was used in this case retrospectively to generate a model with improved nasal projection and dorsal height (Fig. 9). Based upon this model, the actual surface area of tissue required to cover the new nose calculated as 25.8 cm2. This compares to 22 cm2 for the actual flap that was used. The requirement of overexpansion to counteract postoperative contraction and the effect of capsulectomy on postoperative contraction are also future directions of study that may help improve understanding of the behavior of expanded tissue.

Fig. 9. The patient’s preoperative nose was morphed using the Canfield Sculptor software
(Canfield Imaging Systems, A Division of Canfield Scientific Inc, Fairfield, ND, USA),
and the resulting image was measured to deter- mine the size of the flap that would be required to
create a new soft tissue cover for the nose.
LIMITATIONS
The use of 3-dimensional laser scanning and photogrammetry is limited in the head and neck by several factors. Hair-bearing areas cannot be accurately imaged unless shaved. The lower third of the face is constantly in motion and minor differences in the jaw and tongue position can account for several millimeters difference or cubic centimeters of volumetric difference, as seen in Fig. 8. Using a chin rest or even a customized mouth guard in conjunction with a chin rest can be used to overcome this factor if necessary.
SUMMARY
Three-dimensional imaging technology is becoming more readily available and commonly used by reconstructive surgeons. The application of this technology to tissue expansion holds the potential to answer many questions about the planning, expansion, and postoperative phases of reconstruction. Improved understanding of the need for overexpansion, the effect of capsulectomy on contraction, posterior expansion volume, and the bony remodeling that occurs beneath expanders may result from the application of 3-dimensional imaging technology. 3-dimensional morphing and analysis can be used to determine the amount of tissue that will be required to reconstruct a given defect. This area is just now beginning to be explored by clinicians, but holds the promise of allowing reconstructive surgeons to plan and execute complex procedures in the head and neck.
REFERENCES
- Neumann C. The expansion of an area of skin by progressive distension of a subcutaneous balloon. Plast Reconstr Surg 1957;19(2):124-30.
- Swenson RW. Controlled tissue expansion in facial reconstruction. In: Baker SR, editor. Local flaps in facial reconstruction. Philadelphia: Elsevier-Mosby;
2007. p. 667-89. - van Rappard JH, Sonneveld GJ, Borghouts JM.
Geometric planning and the shape of the expander. Facial Plast Surg 1988;5:287. - Brobmann GF, Huber J. Effects of different-shaped tissue expanders on transluminal pressure, oxygen tension, histopathalogic changes and skin expansion in pigs. Plast Reconstr Surg 1985;76(5):731-6.
- Baker SR, Swanson NA. Clinical applications of tissue expansion in head and neck surgery. Laryngoscope 1990;3:100.
- Hsiao C, Hsiao G, Chang L. Accurate assessment of tissue expansion in the lower face and anterior neck by a simple measurement technique. Br J Plast Surg 1999;52:339-42.
- Tepper O, Karp N, Small K, et al. Three-dimensional imaging provides valuable clinical data to aid in unilateral tissue expander-implant breast reconstruction. Breast J 2008;14(6):543-50.
- Moelleken B, Mathes S, Cann C, et al. Long-term effects of tissue expansion on cranial and skeletal bone development in neonatal miniature swine: clinical findings and histomorphometric correlates. Plast Reconstr Surg 1990;86(5):825-34.
- Honrado C, Larrabee WF. Update in three dimensional imaging in facial plastic surgery. Curr Opin Otolaryngol Head Neck Surg 2004;12:
327-31. - Jayaratne YS, Lo J, Zwahlen RA, et al. Three-dimensional photogrammetry for surgical planning of tissue expansion in hemifacial microsomia. Head Neck 2010;32(12):1728-35.
- Ferrario V, Sforza C, Dellavia C, et al. A quantitative three-dimensional assessment of soft tissue facial asymmetry of cleft lip and palate adult patients. J Craniofac Surg 2003;14(5):739-46.
- Ying J, Zhang F, Schwartz J, et al. Assessment of facial tissue expansion with three dimensional digitizer scanning. J Craniofac Surg 2002;13(5): 687-92.
- Weng R, Li Q, Gu B, et al. Extended forehead skin expansion and single-stage nasal subunit plasty for nasal reconstruction. Plast Reconstr Surg 2010; 124(4):1119-28
©2012 Hilger Facial Plastic Surgery