
A Stable, Predictable Technique for Major Dorsal Reconstruction
J. Jared Christophel, MD; Peter A. Hilger, MD
Objective: To assess the long-term stability of osseocartilaginous dorsal onlay rib grafts used for augmentation rhinoplasty.
Methods: Patients who had rib grafts used for augmentation rhinoplasty from 2000 through 2009 were assessed for graft viability, graft mobility, graft warping, maintenance of dorsal projection, functional airway status, need for revision surgery, and donor site morbidity. A retrospective cohort study using telephone follow-up was conducted.
Results: A total of 58 rib graft rhinoplasties were performed in the 10 year review period, 39 of which used dorsal onlay grafts. The mean duration of clinical follow-up was 24 months, and the median duration of clinical follow-up was 16 months. Thirty-three of 33 osseocartilaginous onlay grafts (100%) and 5 of 6 cartilaginous onlay grafts (83%) were viable, rigid, and had maintained dorsal projection at last follow-up. None of the grafts warped. Twenty-nine of 33 patients receiving osseocartilaginous onlay grafts (88%) and 5 of 6 patients receiving cartilaginous onlay grafts (83%) had persisting relief of their nasal obstruction. Twelve of the 39 patients (30%) had revision surgery, mostly performed for minor cosmetic revision.
Conclusions: Osseocartilaginous onlay rib grafts provide an ideal scaffold for dorsal nasal augmentation and restoration of nasal airway in patients with collapse of the nasal framework due to a saddle deformity, history of trauma, or history of multiple septorhinoplasties. The graft has excellent viability, lacks potential for longterm warping, achieves bony fusion to the nasal bones, and allows surgical molding of the cartilaginous tip.
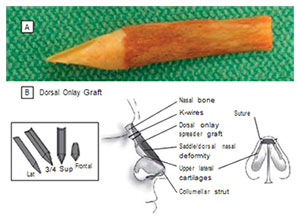
Figure 1. A variation of the cartilaginous rib graft that includes a significant bony portion. A, Carved osseocartilaginous 11th rib graft just prior to implantation. B, Schematic of onlay graft placement. Lat indicates lateral view; Sup, superior view; 3/4, three-quarter view.
ADEQUATE STRUCTURAL AUGMENTATION of the nasal dorsum often requires the use of a rib graft. When performed for revision of the overresected nose, correction of a saddle nose deformity, or severe posttraumatic deformity, the more commonly used grafting materials, such as septal cartilage and auricular cartilage, have either already been used or do not have enough strength to provide the needed support. More rigid graft options include split calvarial bone, autologous rib, irradiated homologous rib, and freeze-dried bone grafts. Of the more rigid grafts available, autologous cartilaginous rib has been the graft of choice for most rhinoplasty surgeons. However, some critics of autologous cartilaginous rib cite its tendency to warp as the biggest potential downside of its use. There have been many attempts to combat this tendency to warp, including concentric carving, setting aside in saline, and internal K-wire fixation. Cartilage also has a higher tendency for resorption, although this risk is low when used in rhinoplasty compared with other areas of facial reconstruction.5 There is also a small risk of mobilization of cartilage grafts because their placement over the bony dorsum allows for fixation with suture only, decreasing the chance of graft integration and increasing the resorption rate. To combat this potential for warping, the senior author (P.A.H.) has used a variation of the cartilaginous rib graft to include a significant bony portion (Figure 1A). As noted, bone is still used for dorsal augmentation by some surgeons, but the choice of optimum source is still debated. Ever since some early publications described the significant resorption of free bone grafts, many surgeons have been hesitant to use it. More recent publications have noted bone used in rhinoplasty to have greater staying power. Specifically, split calvarial bone has become one of the favored grafts because it has lower donor site morbidity and high longterm viability. Ironically, the major benefit of bone grafts is also a big downside: the rigid structure is ideal for the bony dorsum, but it is too rigid for the cartilaginous lower twothirds. The fixation of bone-only grafts has also classically been performed using a cantilevered technique, which is associated with a high rate of screw and/or plate extrusion or showing through the thin skin of the rhinion.
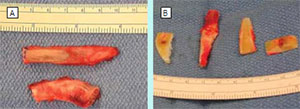
Figure 2. Osseocartilaginous rib graft. A, The 11th osseocartilaginous rib, top, the 10th rib cartilage below. The ruler is in millimeters. B, Unprepared osseocartilaginous 11th rib graft with carved 10th rib cartilage, including notched premaxillary graft on right.
The use of an osseocartilaginous rib graft overcomes many of these obstacles. In following the dictum of Gillies et al, the dorsum is augmented by replacing “like with like”: bone overlies the nasal bones, and cartilage overlies the lower cartilaginous dorsum. The bone over the dorsum allows for bony fusion and integration with the nasal bones and does not have the potential to warp. The cartilage portion at the tip allows the surgeon to carve the implant and to attach the lower lateral cartilages using suture techniques (Figure 1B). Gurley et al10 published a 15-year follow-up study using an osseocartilaginous graft from the fifth to the seventh ribs with excellent results, but many patients still experienced the late effects of hardware used for fixation under the thin skin of the rhinion. The senior author has overcome this obstacle by securing the graft with temporary percutaneous K-wires. Also, the distal 10th rib and floating 11th rib are preferred as graft material because they are thin and easily accessible.
METHODS
PATIENTS

Figure 3. The underside of the onlay graft is hollowed out

Figure 4. The anticipated position of the onlay graft.
Patients who had rib grafts used for augmentation rhinoplasty from 2000 through 2009 were assessed for graft viability, graft mobility, graft warping, maintenance of dorsal projection, functional airway status, need for revision surgery, and donor site morbidity. A retrospective cohort study was performed using a medical chart review and telephone follow-up. A total of 58 rib graft rhinoplasties were performed in the 10-year review period. In 39 of the cases, rib was used as a dorsal onlay graft. These 39 patients created the cohort, of which 33 of the grafts were osseocartilaginous and 6 were cartilage only. The mean duration of clinical follow-up was 24 months. The patients’ mean age was 39 years. Half of the patients had a history of major nasal trauma. Seventy-seven percent of the patients had previous nasal surgery. Of those who had prior surgery, the mean number of procedures was 2.4. All patients presented with nasal obstruction, which was the primary reason for surgical correction.
SURGICAL PROCEDURE
All rib graft rhinoplasties were performed by the senior author and assisted by his fellows. All rhinoplasties were performed using an external approach. Most patients had clinically significant deficiencies in the lower lateral cartilages and dorsal septum with notable scarring of the soft-tissue envelope. The surgery is performed in the following manner. The upper lateral cartilages are separated from the dorsal septum. A subperiosteal dissection pocket is created over the nasal bones, and a 5-mm cutting burr is used to drill down the nasal bones to allow for the increased height provided by the dorsal onlay graft and to allow the graft to sit on bleeding bone for greater bony integration. This burring is also customized to match the undersurface of the dorsal onlay graft to provide a stable platform on which to build the dorsum. The rib graft harvest is begun by selecting an incision site over the floating rib at the inferolateral costal margin. A 5-cm skin incision is used, and dissection is carried down to the fascia of the external oblique fibers, which are spread apart parallel to the direction of the muscle fibers to expose what is often a very thin origin of the internal oblique immediately adherent to the periosteum of the 11th rib. At this point, the rib is assessed for adequate bone stock. In some patients, the 11th rib does not contain enough straight bone length (6 cm) or width (1 cm), and dissection should then proceed using the 10th rib immediately above. The internal oblique fibers are cut parallel to the rib to reveal the underlying periosteum. Two incisions are made in the periosteum of the rib along its superior and inferior borders, preserving the lateral periosteum to be harvested with the rib for possible use as a separate onlay camouflage graft. Circumferential subperiosteal dissection of 6 cm of bone is then performed and transitioned anteriorly to subperichondrial dissection to take at least 2 cm of cartilage of the distal tip.
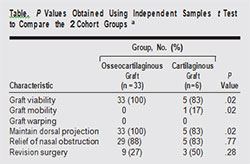
Those who received an osseocartilaginous graft vs those who received a cartilaginous graft. P values represent the likelihood that the difference between the 2 values is due to chance alone.
The cartilage at the tip of the 10th and 11th rib is thin and tapers quickly. In order to have more cartilage for nasal tip grafting, the fused cartilaginous complex of the rib immediately above the osseocartilaginous graft is also harvested (Figure 2A). The anesthesia ventilation circuit is then disconnected, and the lungs are allowed to rest without positive pressure ventilation for 15 seconds. Water is then used to fill the wound, the circuit reconnected, and positive pressure at 30 cm of H2O held to ensure that there is no pleural leak. The wound is then closed in layers, closing the periosteal envelope where possible, reapproximating the internal oblique muscle/fascia, deep dermis, and finally skin. An On-Q pain pump (I-Flow Corp, Lake Forest, California) and an active 19 French round Jackson Pratt drain are placed prior to closure. The osseocartilaginous rib graft is then burred down on the undersurface to create a hollow dugout that will saddle the nasal bones (Figure 3). The graft is then inserted as a dorsal onlay graft and seated onto the nasal bones. The anticipated position is shown in Figure 4. The stability of the interface between the nasal bones and undersurface of the graft is assessed, and the graft is removed and the interface contoured as needed with the burr to provide a stable platform. Any dorsal contour abnormality is noted, and the burr used to remove any dorsal irregularity.
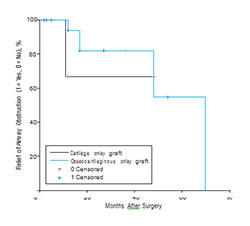
Figure 5. Kaplan-Meier survival analysis of relief of airway obstruction. Survival probability refers to maintenance of nasal obstruction.

Figure 6. Patient 1. Lateral views before (A) and after (B) surgery.
An important note needs to be made about osteotomies given that this technique relies on a stable bony dorsum. If there is only a mild dorsal deviation, osteotomies are deferred because the onlay graft can camouflage minor deformities. However, in many posttraumatic noses, the bony deviation is clinically significant and contributes to the nasal airway obstruction. In these cases, osteotomies are performed using techniques that preserve periosteal attachments such as the postage stamp technique. Achieving stable contact of the bony portion of the graft to the bony dorsum is paramount. Most of these patients have had severe loss of septal structure, and short of a septal replacement graft, it is not possible to provide any meaningful support to an onlay graft from the underlying septum. Moreover, the stability offered by this integrated and stable graft is superior to that of a graft that is not integrated into the bony dorsum and depends on a slender pillar of cartilage in the midline dorsum. Once the graft is seated in the appropriate location, the upper lateral cartilages are then sewn to the outer edges of the onlay graft, which functions as an onlay spreader (Figure 1B). Drill holes with a 1.5-mm drill are made if needed in the lateral edges of the graft to accept 5-0 PDS suture. Affixing the upper lateral cartilages secures the graft in a stable position, and then further trimming of the cartilaginous tip can be performed as necessary and the lower lateral cartilages affixed with 5-0 PDS in the desired position. Usually, the dorsal onlay graft is cantilevered off the bony dorsum of the nose and sufficiently stable. However, when the soft tissues of the lower third of the nose are severely contracted, the cantilever graft may require reinforcement with an articulated columellar strut. This is particularly true when scarred vestibular lining limits nasal tip projection. In some of the severely decimated noses, a premaxillary graft is needed both to fill out the retracted columellar/labial angle and to provide a foundation on which to build the columella. These are fairly sizable grafts made from the extra cartilaginous rib (taken from the cartilaginous rib immediately above the osseocartilaginous graft) and extend across the width of the alar base (Figure 2B). They are placed through the columellar dissection and interdigitated with the anterior nasal spine. If necessary, this graft too can be temporarily stabilized with percutaneous K-wires that engage the premaxilla. Additional sidewall, alar, or columellar grafting is then performed with the extra cartilaginous rib if needed. Once all grafts are in place, the soft-tissue envelope is redraped and 2 percutaneous K-wires are placed through the skin of the rhinion, through the graft, and into the nasal bones. The K-wires are trimmed to the level of the skin and removed in clinic 3 weeks after surgery once the graft has fused to the nasal bones. A postoperative chest radiograph is obtained in all patients to ensure that there is no occult pneumothorax. Patients are admitted overnight, discharged on postoperative day (POD) 1, and return to have the drain and On-Q pump removed on POD 3.
FOLLOW-UP
Patients were assessed at 1 week, 3 weeks, 3 months, 6 months, and 12 months postoperatively. Patients traveling from other countries were not followed in clinic for more than 3 weeks. At each visit, the dorsal onlay grafts were assessed for resorption, mobility, or warping by examination. Standard rhinoplasty photographs were taken beginning at the 3-week visit. Profile views were used to assess maintenance of dorsal projection beginning at the 3-month time mark once most of the edema had subsided. Beginning at the 3-month visit, patients were assessed for relief of nasal obstruction at each visit. The validated Nasal Obstruction Symptom Evaluation (NOSE) survey has been instituted in the past few years; however, to allow comparison with earlier patients, relief of nasal obstruction was divided into a binary outcome of improved vs not improved.
RESULTS
A total of 58 rib graft rhinoplasties were performed in the 10-year review period. All patients who had dorsal onlay rib grafts were evaluated as a cohort (39 patients), and classified according to graft type: osseocartilaginous rib grafts (33 patients) and cartilaginous rib grafts (6 patients). The mean duration of clinical follow-up was 24 months (median duration, 16 months). Thirty-three of 33 osseocartilaginous onlay grafts (100%) and 5 of 6 cartilaginous onlay grafts (83%) were viable and rigid at the last follow-up (1 cartilage graft resorbed). None of the grafts warped. None of the patients who underwent osseocartilaginous graft had lost dorsal projection. Twenty-nine of 33 patients who underwent osseocartilaginous graft (88%) and 5 of 6 of those who underwent cartilaginous onlay graft (83%) had persisting relief of their nasal obstruction with a mean duration of follow-up of 24 months. Twelve of 39 patients (30%) had revision surgery, 5 cases of which were for recurrent nasal obstruction and 7 for minor cosmetic revision. There were no pneumothoraces. One patient had prolonged chest wall discomfort that lasted 6 weeks. See the Table for a summary. The difference in the graft viability between the osseocartilaginous and cartilaginous onlay grafts was significant (P = .02) using an independent-samples t test and assuming equal variances. The slight difference in persisting relief of airway obstruction between the 2 graft types was not significant (P = .77). While using a means test (t test) may be informative regarding different rates of graft survivability, the statistic of persisting relief of airway obstruction (the primary reason for the surgery) warrants further investigation. Most of the patients who presented with recurrent nasal obstruction did so after 24 months. Of those who experienced a recurrence, the mean time to recurrence was 22 months after surgery. If viewed at the 12-month mark, all but 1 patient noted persisting relief of nasal obstruction. To better analyze the recurrence of nasal obstruction in a population in which follow-up is not constant and the time to event (recurrence) is variable, the Kaplan-Meier survival analysis was applied (Figure 5). This gives a better analysis of a late complication occurring outside of the usual follow-up window because it accounts for patients and their status at the last known follow-up. This method reveals a 74% chance of maintenance of nasal airway at 48 months, down from the 87% when analyzing the nasal airway in a mere yes/no fashion at the last follow-up. This number is lower because late follow-up could not obtained in patients who were released from care at 12 months without complications. Of note, when analyzing the “survival” of the nasal airway factored on graft type (osseocartilaginous vs cartilaginous), there was no significant difference between the 2 based on a log Rank test (P = .61).

Figure 7. Patient 2. Preoperative (A) and 3-month postoperative (B) frontal views. Preoperative (C) and 3-month postoperative (D) lateral views.

Figure 8. Patient 3. Lateral views before (A) and after (B) surgery.

Figure 9. Patient 4. Lateral views before (A) and after (B) surgery.

Figure 10. Patient 5. Lateral views before (A) and after (B) surgery.
PATIENT 1
A 36-year-old man from France had experienced nasal trauma as a child (Figure 6). He had undergone external septorhinoplasty in France when was in his 20s and developed septal perforation and saddle deformity. The dorsum was reconstructed using an osseocartilaginous 11th rib graft. Figure 6B is from the 3-month postoperative follow-up. A telephone follow-up performed 24 months after surgery revealed persisting relief of airway obstruction and excellent subjective cosmetic results.
PATIENT 2
A 63-year-old man had previously undergone external septorhinoplasty with overresection and developed intranasal synechiae with nasal obstruction (Figure 7). The dorsum was reconstructed with an osseocartilaginous 10th rib graft. Figure 7B and D show the patient 3 months after surgery. Anterior views reveal changes to brow tip aesthetic line. The 12-month telephone follow-up revealed persisting relief of airway obstruction and excellent subjective cosmetic results.
PATIENT 3
A 26-year-old man with a history of multiple sportsrelated nasal traumas (Figure 8). He had previously undergone septoplasty for nasal obstruction and developed saddle deformity and persisting nasal obstruction. The nasal dorsum was reconstructed with an osseocartilaginous 11th rib graft. The follow-up photograph (Figure 8B) shows the patient at 4 months after surgery. The telephone follow-up at 24 months revealed persisting relief of airway obstruction and excellent subjective cosmetic results.
PATIENT 4
A 43-year-old man with a history of nasal trauma and subsequent external septorhinoplasty (Figure 9) developed loss of projection and nasal tip ptosis with nasal obstruction. The dorsum was reconstructed with an osseocartilaginous 11th rib graft. Figure 9B shows the patient 41 months after surgery. An excellent nasal airway has been maintained.
PATIENT 5
A 53-year-old man with a history of nasal trauma and subsequent septoplasty to relieve nasal obstruction (Figure 10) developed saddle nose and recurrent nasal obstruction. The dorsum was reconstructed with an osseocartilaginous 11th rib graft. Figure 10B shows the patient at the 12-month follow-up. The clinical follow-up at 24 months revealed an excellent cosmetic result and persisting relief of nasal obstruction.
COMMENT
The osseocartilaginous rib graft has proven to be a superior graft when performing major dorsal augmentation. To date, of the 33 osseocartilaginous grafts used there has been no resorption, mobilization, or warping. It is interesting to note the statistically significant difference in graft survival between the osseocartilaginous and cartilaginous rib grafts. The senior surgeon prefers osseocartilaginous rib grafts but will use cartilaginous grafts from the fifth, sixth, or seventh rib as a second option, usually in females, when patients do not want a inferolateral chest wall scar. This provided us the opportunity to perform a retrospective cohort study of all patients receiving dorsal onlay rib grafts. One would assume that the single resorbed cartilaginous graft was due to chance. However, the statistical significance in difference in graft viability gives strength to the argument supporting the use of an osseocartilaginous graft when possible.
It was also interesting to note the late presentation of recurrent nasal obstruction in these patients. It is usually taught that most postoperative healing and contraction in rhinoplasty will be complete by 12 months, but this does not explain our results. Four of 5 of these patients experienced recurrence of the nasal obstruction because of internal valve stenosis after the 12-month mark, which was corrected with an endonasal revision with either batten graft placement or composite graft to relieve a cicatricial scar. In all of these cases, the dorsal onlay graft was stable and did not contribute to the recurrent vestibular stenosis. Nonetheless, these results emphasize the importance of following patients who undergo major dorsal reconstruction beyond the 12month mark.
One of the more difficult hurdles in major dorsal augmentation lies in expanding a contracted soft-tissue envelope. This is more easily accomplished with the outer skin envelope; however, a contracted lining is very difficult to correct. Often the retracted upper lateral cartilages have difficulty reaching the lateral aspect of onlay spreader. This force of contraction is likely what underlies the late presentation and internal valve stenosis in most patients. To combat the retraction of the upper lateral cartilages in patients with a collapsed middle vault, the osseocartilaginous graft can be fashioned such that the bony portion extends further caudally. This allows the upper lateral cartilages to be affixed to a greater component of bone as the bonycartilaginous junction usually occurs in the middle vault. Of note, the overall rate of revision surgery for these patients is higher (30%) than usual for rhinoplasty. Whether this is due to the revision nature of these rhinoplasties or to the technique is hard to tell, but most of the revisions were for minor refinements (eg, rasping of a dorsal irregularity).
The fundamental strength of the osseocartilaginous rib graft lies in replacing like with like. When major dorsal augmentation is performed, cartilage or bone grafts are required to masquerade as either bone or cartilage at some point along the dorsum, depending on the graft used. A chimeric bony and cartilaginous graft allows for bony integration with the nasal dorsum, preventing mobilization, and allows for fine sculpting of the cartilaginous nasal tip.
Accepted for Publication: September 23, 2010.
Published Online: November 15, 2010. doi:10.1001/archfacial.2010.95
Correspondence: J. Jared Christophel, MD, Department of Otolaryngology–Head and Neck Surgery, Division of Facial Plastic Surgery, University of Virginia Health System, PO Box 800713, Charlottesville, VA 22908 ([email protected]).
Author Contributions: Study concept and design: Christophel and Hilger. Acquisition of data: Christophel. Analysis and interpretation of data: Christophel and Hilger. Drafting of the manuscript: Christophel. Critical revision of the manuscript for important intellectual content: Christophel and Hilger. Statistical analysis: Christophel. Administrative, technical, and material support: Christophel and Hilger. Study supervision: Hilger.
Financial Disclosure: None reported.
Previous Presentation: This study was presented as an oral presentation at the 10th International Symposium of Facial Plastic Surgery; April 28, 2010; Hollywood, Florida.
REFERENCES
- Gunter JP, Clark CP, Friedman RM. Internal stabilization of autogenous rib cartilage grafts in rhinoplasty: a barrier to cartilage warping. Plast Reconstr Surg.
1997;100(1):161-169. - Hiraga Y. Complications of augmentation rhinoplasty in the Japanese. Ann Plast
Surg. 1980;4(6):495-499. - Daniel RK. Rhinoplasty and rib grafts: evolving a flexible operative technique.
Plast Reconstr Surg. 1994;94(5):597-611. - Adams WP Jr, Rohrich RJ, Gunter JP, Clark CP, Robinson JB Jr. The rate of warping in irradiated and nonirradiated homograft rib cartilage: a controlled comparison and clinical implications. Plast Reconstr Surg. 1999;103(1):265-270.
- Tardy ME Jr, Denneny J III, Fritsch MH. The versatile cartilage autograft in reconstruction of the nose and face. Laryngoscope. 1985;95(5):523-533.
- Chase SW, Herndon CH. The fate of autogenous and homogenous bone grafts.
J Bone Joint Surg Am. 1955;37(4):809-841. - Mowlem R. Bone grafting. Br J Plast Surg. 1963;16:293-304.
- Thomassin JM, Paris J, Richard-Vitton T. Management and aesthetic results of support grafts in saddle nose surgery. Aesthetic Plast Surg. 2001;25(5):332-337.
- Sajjadian A, Rubinstein R, Naghshineh N. Current status of grafts and implants in rhinoplasty, part I: autologous grafts. Plast Reconstr Surg. 2010;125(2):40e-49e.
- Gurley JM, Pilgram T, Perlyn CA, Marsh JL. Long-term outcome of autogenous rib graft nasal reconstruction. Plast Reconstr Surg. 2001;108(7):1895-1907.
- Gillies HD, Fry WK, Wade H. Plastic Surgery of the Face Based on Selected Cases of War Injuries of the Face Including Burns With Original Illustrations. London, England: H Frowde; 1920.
- Clark RP, Wong G, Johnson LM, et al. Nasal dorsal augmentation with freezedried allograft bone. Plast Reconstr Surg. 2009;124(4):1312-1325.
- Byrne PJ, Walsh WE, Hilger PA. The use of “inside-out” lateral osteotomies to improve outcome in rhinoplasty. Arch Facial Plast Surg. 2003;5(3):251-255.
©2012 Hilger Facial Plastic Surgery