
ANTHONY E. BRISSETT, MDA, PETER A. HILGER, MDB
- Unique characteristics
- Presurgical evaluation
- Procedures
- Incisions
- Surgical techniques
- Adjunctive procedures
- Summary
- References
To live longer and look better, men and women maintain their health and wellness by modifying their diet, exercising, and avoiding deleterious activities such as smoking or alcohol consumption. Although these lifestyle adjustments can help to maintain or improve health, there is often a disconnection between how people may feel on the inside and their outward appearance. With the advent of nonsurgical interventions such as Botox and injectable fillers, as well as newer less invasive surgical techniques, cosmetic procedures and facial rejuvenation are increasing in popularity. The most common motivator for men and women interested in cosmetic surgery is to look younger and improve their appearance; however, men are twice as likely as women are to undergo cosmetic procedures for anticipated work-related benefits [1]. A review of 2003 cosmetic surgery statistics revealed that men accounted for 14% of the nearly 9 million cosmetic procedures performed in the United States [2].
Middle-aged men represent an emerging group expressing an interest in facial rejuvenation procedures. One must understand the complex differences in the male patient’s motivation, psychosocial factors, and the unique aspects associated with anatomy and facial aging. To maximize postoperative results and increase patient satisfaction, the facial plastic surgeon must adjust perioperative management and surgical techniques when per- forming a male facelift.
UNIQUE CHARACTERISTICS
Although the objectives of a facelift are the same for men and women, the facial plastic surgeon must consider additional characteristics that are unique to male patients. These characteristics include differences in the process of aging, as well as a multitude of anatomic and psychosocial factors [3–6].
When evaluating changes in the face that occur over time, men often identify different areas of concern when compared with women. Men tend to have increased concerns about their midface and neck, whereas women are often concerned with their upper face in addition to their midface and neck [7]. In men, there is a greater degree of descent of the melolabial mound leading to increased midfacial hollowing and more pronounced nasolabial folds. In addition, the amalgamation of thick and heavy redundant skin, excess submental fat, and dehiscent platysmal musculature leads to the appearance of heaviness in the neck, which is often much worse in men. These differences necessitate careful and thoughtful consideration when preparing men for facelift surgery and underscore the divergence between men and women with respect to facial aging.
One of the greatest issues when considering facelift surgery in men is the specific pattern and distribution of facial and temporal hair. In men, there is an area of hairless skin between the sideburn and the ear. If this hairless area is not preserved at the time of surgery or reestablished postoperatively, hairbearing skin will be displaced onto the preauricular area and tragus. Care should be taken in patients who have extreme skin laxity, because the lifting process may result in the partial or complete excision of sideburns. In addition, during the lifting process, part of the bearded skin is often displaced posteriorly, potentially relocating hairbearing skin onto the back of the ear. When planning the incision, the facial plastic surgeon must also consider the hair distribution in the temporal area, as well as the presence of, or potential for, male pattern baldness.
The male patient presents with three basic hair distribution patterns in the temporal area: (1) a normal full growth of hair, (2) thinning hair with temporal recession, or (3) significant male pattern baldness [3]. Anything other than a normal full growth of hair necessitates incision modification in the temporal area.
When considering facial rejuvenation procedures in men, the surgeon should recognize that fundamental differences exist in their motivation, expectations, support systems, and adaptability to changes in appearance. Women tend to be more accustomed to periodic changes in their facial appearance. This level of comfort is often achieved through routine changes to their hairstyle or color, as well as by varying make-up. As a result, women are often more accepting and realistic about changes in facial appearance.
For men, the first opportunity to review their facial appearance may occur during the initial office consultation with the facial plastic surgeon. The male patient’s expectations and ability to accept changes in his appearance following surgery may result in a greater difficulty with lifestyle transition when compared with the adaptability of a female patient. Given that men are often less expressive, it is essential that the facial plastic surgeon engage them in a detailed discussion surrounding their specific expectations. At this time, the psychiatric profile of male patients considering facial rejuvenation procedures should be explored in an attempt to identify those with possible body dysmorphic disorders or unrealistic expectations.
Men may have different overall health issues and cardiac risk factors when compared with women of similar age. The increased incidence of cardiovascular and pulmonary diseases in men necessitates a careful preoperative assessment. The use of tobacco or nicotine-containing products, vitamins with anticoagulant effects, or nonsteroidal anti-inflammatory agents must be determined. It is essential that the facial plastic surgeon identifies all of these issues preoperatively and coordinates the patient’s care with an internist or primary care provider to minimize the risk for myocardial infarction, pneumonia, flap necrosis, and hematoma.
PRESURGICAL EVALUATION
The facial plastic surgeon must appreciate the unique needs of the male patient who desires a more youthful appearance and create an environment that facilitates an effective and realistic outcome. Because men have different experiences and expectations related to facial rejuvenation procedures and cosmetic surgery, the facial plastic surgeon should provide structure and support during the consultation and perioperative period.
During the initial visit, the patient’s esthetic concerns, motivations, and expectations should be explored. This information will allow the facial plastic surgeon to discuss the variety of factors specific to the needs of the patient and to customize the procedure to best suit the patient. The patient and surgeon should evaluate preoperative and postoperative photographs during the initial consultation. By reviewing photographs, the patient can obtain a better understanding of realistic postoperative outcomes. The focus should then shift to the evaluation of the patient’s face. Computer image analysis enhances this portion of the consult because the patient can carefully evaluate his facial characteristics from multiple views. During this process, the surgeon should perform a complete facial evaluation, including an analysis of the skin and underlying bony structures, as well as an assessment of the forehead, eyebrows, mid- face, and neck. Once this evaluation is complete, the patient and surgeon can begin to develop a comprehensive plan for facial rejuvenation.
If the need for multiple procedures is recognized, a priority list can be created to assist the patient in formulating a realistic plan. Although women often undergo multiple facial rejuvenation procedures simultaneously, it may be more suitable for men to undergo facial rejuvenation procedures in a staged fashion. Doing so allows patients to have time to adjust to subtle changes in their appearance rather than facing radical changes that may occur when multiple procedures are performed simultaneously. Once this overview has been provided, patients are given reading materials and pamphlets related to their desired procedures and are encouraged to review them carefully before returning for their second consultation.
Multiple office consults are often needed when formulating a surgical plan for the male patient. During these consultations, a detailed discussion related to the advantages and disadvantages of facelift procedures should take place. Issues such as scarring, hypesthesia, displacement of hair, and numbness should be pointed out. The potential need for postoperative ancillary procedures should be mentioned.
PROCEDURES
INCISIONS
A major difference when planning a facelift in men relates to the placement of incisions. The three major areas that necessitate variations when planning incisions include the superior portion of the incision within the temple, the anterior segment of the incision located in the preauricular area, and the posterior aspect of the incision, including postauricular, mastoid, and occipital extensions [3]. When planning the temporal incision, the most important consideration is to minimize alterations in the hairline and maintain the temporal tuft of hair. For patients with a full growth of hair and no temporal recession, no significant modification of the incision is necessary. The upper portion of the incision can be extended superiorly into the temple, or can begin inferiorly to follow the temporal tuft or hair line slightly above the helical root [Fig. 1A,B] The presence of thinning hair with temporal recession or significant male pattern baldness necessitates modifications of the upper segment of this incision. The superior incision may require shortening to prevent it from extending into the area of recessed hair. Alternatively, the vertical portion may need to be eliminated. The advantages of creating a horizontal extension, inferior to the temporal hairline, are that it maintains the temporal tuft and prevents its recession or elevation. Additionally, the horizontal extension allows bearded hair to be moved superiorly to recreate the sideburn, if necessary.
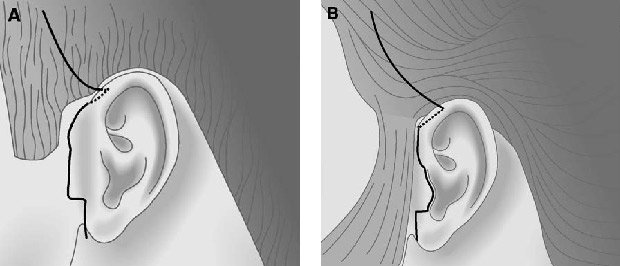
Fig. 1. Temporal and preauricular incision placement. (A) The superior portion of the incision extends into the temporal area. The preauricular incision may be placed behind the sideburns. (B) Superior extension may vary depending on the temporal hairline. In the posttragal approach, the incision should be placed within the zone of color transition at the junction of the helix and the cheek. A 2-mm rim of tissue is preserved at the ear lobe.
Another area of consideration in men undergoing a faceliftis the anterior segment of the incision located in the preauricular area. The dilemma associated with the anterior incision in men is preserving the non–hair-bearing skin in the preauricular area while maintaining the proper location of side- burns. For women, there are two variations of this anterior incision. The first involves placing the incision entirely in the preauricular sulcus. The second involves creating a retrotragal incision [8].
In men, the preauricular incision can be placed directly in front of the non–hair-bearing area [Fig. 1A]; however, the drawback with this approach is the potential for a more conspicuous scar. An additional option is to place the incision in the preauricular sulcus with a posttragal extension, similar to that used in women [Fig. 1B]. Although this second option may result in a less obvious scar, it may also result in the displacement of hair-bearing skin onto the tragus, eliminating the natural area of hairlessness in the preauricular area. The decision related to the placement of the anterior portion of the incision is a matter of personal preference for the surgeon. A 2-mm cuff of tissue should be preserved as the incision proceeds around the ear lobe. This cuff prevents displacing hair-bearing skin into the preauricular sulcus, creating difficulty when shaving. The facial plastic surgeon should be cognizant of the skin color changes that occur in the preauricular area and should place incisions within the junction of the color change, regardless of which approach is used [4].
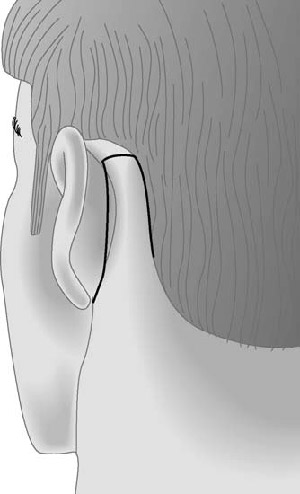
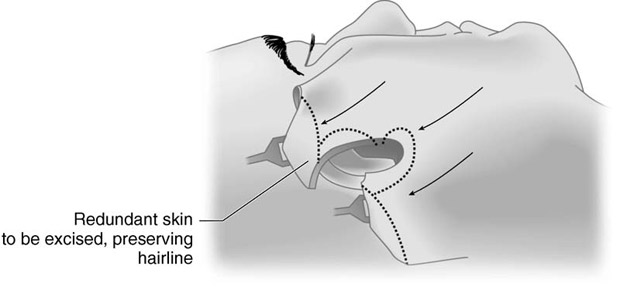
FlG. 2. Posterior and occipital incision placement. The posterior aspect of the incision should be placed within the cephaloauricular groove. The occipital extension can be placed in a pretrichial position.
The posterior aspect of the facelift incision includes the postauricular, mastoid, and occipital extensions and is the third area that requires modification [3]. In women, this incision typically runs superiorly along the posterior aspect of the concha and then extends posteriorly into the hairline. If this incision is maintained in men, it may draw hair-bearing skin onto the posterior aspect of the ear, necessitating shaving. To prevent this displacement, it is best to place the incision within the cephaloauricular groove [Fig. 2]. In addition, ex- tending the posterior incision into the hairline may result in displacement of the hairline as well as contour irregularities. To minimize posterior and superior hairline displacement as well as stair stepping in the male patient, it may be advantageous to place the incision in a pretrichial position along the inferior aspect of the hairline.
SURGICAL TECHNIQUES
In the preoperative holding area, all incision lines, anatomic landmarks, fat accumulations, and platysmal bands should be marked. To achieve the most accurate estimation of tissue, all markings should be completed when the patient is awake and sitting upright. Once the patient moves into a supine position, the tissue assumes a more superior and posterior location, making the landmarks and markings less accurate. The preoperative markings should include the planned incision lines, the gonial angle, the inferior border of the mandible, and the origin of the zygomaticus major muscle. The origin of the zygomaticus major muscle can be identified by palpating the slight indentation on the zygoma at the malar eminence.
The use of various anesthetic options is a matter of surgeon and patient preference. Ideally, facelift operations are performed under general endotracheal anesthesia as opposed to intravenous sedation with monitored anesthesia care. Owing to the increased likelihood of bleeding in male patients, the use of intravenous sedation with local anesthesia may result in some lability of blood pressure, increasing the likelihood of intraoperative bleeding and postoperative hematoma. The tube should not be taped to the lower lip or chin, because this will create difficulty when accessing the submental area and neck. If the tube is secured to the skin of the chin and mandible, it will resist the vectors of pull required for adequate face and neck-lifting. The tube can be secured by passing a 0-silk suture through the interdental space of the maxillary central incisors, securing it first to the teeth and then around the tube. In this fashion, access to the neck and submental area is facilitated while minimizing the potential for extubation. Once general anesthesia has been induced, the next step is to inject the facial and scalp incisions on the face and neck with 0.25% lidocaine with 1:100,000 epinephrine. This dilution allows for the safe injection of volume required for appropriate local anesthesia and hemostasis.
If submental liposuction or fat sculpturing is to be performed, this aspect is completed first through a submental incision. It is critical to stay in the supraplatysmal plane to avoid injury to major vessels and the ramus mandibularis. In the midline, care must be taken because the platysmal muscle is frequently dehiscent and laterally displaced, making the central anterior jugular vein vulnerable to injury. Submental fat can be removed with sharp excision or suction techniques. In some instances, subplatysmal fat may accumulate medially and require sharp excision. The removal of excess fat from the underside of the skin flap as well as in the area of the submental crease should be avoided. If the subcutaneous fat beneath the skin flap in the neck is aggressively resected, scar formation and adherence of the skin to the underlying platysmal muscle is likely to occur. This adherence prevents the skin from gliding over the platysma muscle during facial expression or swallowing, creating a displeasing and unnatural appearance. Once adequate liposuction and sculpting have been completed, the me- dial border of the platysma should be identified and exposed to the level of the thyroid notch inferiorly. Platysmal plication can then be performed with interrupted 4-0 Vicryl sutures. If the platysmal muscle is hypertrophic and thick, it may be beneficial to trim the medial edges before plication. When the incision is made in the posterior hairline, the surgeon should bevel the incision to allow hair to grow through it. The occipital skin flaps should be elevated posteriorly and inferiorly for several centimeters. The sternocleidomastoid muscle creates cutaneous attachments that must be re- leased during flap elevation. Care must be taken to stay above this muscle to minimize potential injury to the great auricular nerve and external jugular vein. The extent of occipital undermining is determined by the laxity of the lower neck skin; if large amounts of lower neck skin need to be redraped, more extensive undermining will be required.
The deep plane technique is the procedure of choice for men undergoing a facelift. The advantages of this procedure include minimizing the closing tension placed upon the skin, elevation of the melolabial fat pad, effacement of the jowls, and sharpening of the cervical facial angle. The sequence of events for the deep plane technique is as follows:
- Elevation of preauricular and occipital skin flaps
- Superficial musculoaponeurotic system (SMAS) incision and anterior dissection
- Release of cutaneous ligaments
- Blunt dissection into the malar fat pad
- Release of platysmal musculature
- Elevation and suspension of the SMAS and platysma
- Trimming and inset of preauricular and occipital skin
In the midface and neck skin of men, the presence of hair follicles creates a richer and more robust subdermal plexus. This characteristic may increase bleeding, escalating the likelihood of a hematoma as well as creating difficulties in establishing the appropriate plane of dissection. Additionally, to prevent damaging the hair follicles, a greater amount of subcutaneous fat should remain on the undersurface of the flap. Anterior elevation of the skin flap is performed for approximately 3 cm in a subcutaneous plane and should be elevated inferiorly, stopping approximately 1 cm above the inferior border of the mandible.
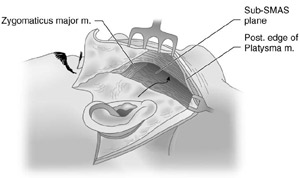
FlG. 3. Sub-SMAS midface dissection. Male Face-Lift 455
Skin flap elevation in the lower neck should then proceed in the supra-SMAS plane. Once the skin flaps have been elevated, the SMAS can be raised in the midface and for a short duration in the neck. In the midface, an incision is made in the SMAS extending from the root of the helix to the angle of the mandible [Fig. 3]. Blunt dissection is used to elevate the SMAS flap anteriorly to the nasolabial fold. The dissection is carried inferiorly, stopping approximately 1 cm above the inferior border of the mandible. Once the SMAS flap has been completed, a supra-SMAS dissection should be started beginning at the level of the zygomaticus major muscle. Dissection can then follow the superficial aspect of the zygomaticus major toward the modiolus, resulting in release of the zygomaticus cutaneous and masseteric cutaneous retaining ligaments as well as separating the malar fat from the deep tissue of the midface [9]. The subplatysmal dissection should be completed in the neck below the level of the mandible. Limited subplatysmal dissection can proceed for approximately 1 to 2 cm anteriorly without encountering the marginal or cervical branches of the facial nerve.
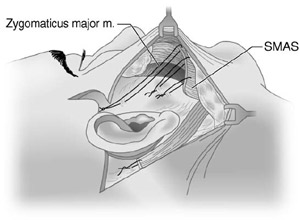
FlG. 4. SMAS and platysmal suspension. A 2-0 polydioxanone suture is used to suspend the superior aspect of the SMAS to the deep temporalis fascia. The inferior aspect of the SMAS is transposed posteriorly, elevated, and fixated to the mastoid fascia.
The SMAS and platysmal flaps require elevation and posterior advancement. This maneuver elevates the midface and malar fat pad while minimizing the closing tension on the overlying skin and sharpening the cervical facial angle. The excess SMAS within the midface is approximated and excised in a superior to inferior fashion. During this portion of the procedure, the authors leave a small amount of the SMAS tethered to the platysmal muscle inferiorly. This portion of tissue is then transposed posteriorly and sutured to the mastoid fascia to accentuate the neck-lift and sharpen the cervical facial angle. Fixation of the SMAS and platysma occurs in posterior and superior vectors. The SMAS flap is secured to the deep temporal fascia with a 2-0 polydioxanone suture. Additional sutures are then placed along the preauricular area. The inferior portion of the SMAS and the platysmal flap are then advanced behind the ear and secured to the mastoid fascia [Fig. 4]. The platysma should be plicated to the anterior border of the sternoclei- domastoid muscle. At this stage, adequate hemostasis should be confirmed, and drains should be placed in the postauricular scalp, extending inferiorly over the sternocleidomastoid muscle. The use of suction drains may be obviated with the use of growth factors or tissue adhesives [10].
FlG. 5. Skin trimming and flap inset. Skin is trimmed at the temporal tuft, preauricular area, and occipital extension. Hair bulbs may require trimming if a retrotragal incision is used.
Before any trimming of skin, it should be redraped and the postauricular hairline restablished to ensure that step deformities are minimized or eliminated. Superior advancement of the skin flaps often results in the development of redundant tis- sue and standing cone deformities in the area of the temporal tuft. This tissue will need to be removed by excising redundant skin inferior to the temporal tuft [Fig. 5]. This technique preserves the relation- ship of the sideburns to the temporal hairline. Because of the thickness of skin in men, the skin of the neck may gather or bunch and will not redrape as well as the thinner more pliable skin in women. In addition, weathered or sun damaged skin may have irregularities that the surgeon should be attentive to during the process of skin advancement and redraping.
To avoid the shift of bearded skin into the hair- less preauricular area, the hair follicles on the undersurface of the flap can be excised or cauterized with needle point cautery [4]. The preauricular skin is closed in layers using a 5-0 Vicryl and 6-0 nylon suture. If a retrotragal incision is used, the pretragal hollow must be re-established with a dermal stitch. This maneuver recreates the normal preauricular contour and prevents flaring of the tragus.
The posterior portion of the flap is then trimmed, redraped, and closed with a nylon suture. The occipital extension is closed with staples, and a large bulky pressure dressing is applied. All patients should receive a course of antibiotics, appropriate analgesics, and antiemetics if indicated. All patients should be seen on the first postoperative day for dressing removal, wound inspection, and drain removal. An elastic support style dressing can then be worn intermittently for the next 48 to 72 hours. Stitches and staples are removed within 7 to 10 days. During the first postoperative week, male patients who undergo facelift procedures may require increased support. The surgeon and staff should be sensitive to this and be prepared to respond with frequent phone calls or office visits.
ADJUNCTIVE PROCEDURES
In some male patients seeking facial rejuvenation, additional procedures may be indicated to obtain a harmonious youthful appearance [Fig. 6]. In some cases, a forehead-lift, blepharoplasty, rhinoplasty, midfacial implants, or chin augmentation may be necessary. Botox may be indicated postoperatively to address dynamic wrinkles in the periorbital and glabellar regions. The deep plane facelift technique is often ineffective at effacing the melolabial fold [11]; as a result, injectable fillers may be required to soften this area. If bearded hair has been transferred into the preauricular area, laser depilation may be needed to re-establish the preauricular zone of hairlessness.

Fig. 6. Pre- and postoperative results. (A, B) Preoperative photographs of a 56-year-old man with signs of facial aging. (C,D) Postoperative photographs following an endoscopic brow-lift, upper lid blepharoplasty, lower lid blepharoplasty, deep plane face-lift, submental liposuction, and platysmal plication.
SUMMARY
Middle-aged men represent a unique group expressing increased interest in facial rejuvenation procedures. Although the objectives of a facelift are the same for men and women, the facial plastic surgeon must consider additional characteristics that are unique to male patients, including differences in the process of aging, as well as a multitude of anatomic and psychosocial factors. The facial plastic surgeon should consider all of these factors when preparing for a facelift procedure in men.
REFERENCES
- American Academy of Facial Plastic and Recon- structive Surgery. American Academy of Facial Plastic and Reconstructive Surgery 2003 member- ship survey: trends in facial plastic surgery. Alexandria (VA): American Academy of Facial Plastic and Reconstructive Surgery; 2004.
- American Society of Plastic Surgeons. 2003 Gen- der distribution cosmetic procedures. Available at: http://www.plasticsurgery.org/public_education/ loader.cfm?url=/commonspot/security/getfile. cfm&PageID=13620. Accessed March 21, 2005.
- Botta SA. Face lifts in male patients. Facial Plast Surg 1992;8:72–8.
- Connell B. Male face lift. Aesthetic Surg J 2002; 22:385–96.
- Cremone J, Courtis EH, Baker Jr JL. Male rhyti- dectomy incisions. Plast Reconstr Surg 1983;71: 423–6.
- Papel ID, Lee E. The male facelift: considera- tions and techniques. Facial Plast Surg 1996;12: 257–63.
- Smith JW, Nelson R, Weaver K. Rhytidectomy in male patients. Aesthetic Plast Surg 1983;7: 41–5.
- Becker FF. The preauricular portion of the rhyti- dectomy incision. Arch Otolaryngol Head Neck Surg 1994;120:166–71.
- Sherris DA, Larrabee Jr WF. Anatomic considera- tions in rhytidectomy. Facial Plast Surg 1996;12: 215–22.
- Brissett AE, Hom DB. The effects of tissue sealants, platelet gels, and growth factors on wound healing. Curr Opin Otolaryngol Head Neck Surg 2003;11:245–50.
- Hamra ST. A study of the long-term effect of malar fat repositioning in face lift surgery: short- term success but long-term failure. Plast Reconstr Surg 2002;110:940–59.
a Facial Plastic and Reconstructive Surgery, Bobby R. Alford Department of Otorhinolaryngology/Head and Neck Surgery, Baylor College of Medicine, 6550 Fannin, Suite 1701, Houston, TX 77030, USA
b Division of Facial Plastic Surgery, Department of Otolaryngology/Head and Neck Surgery, University of Minnesota, 5050 France Ave S, Suite 150, Edina, MN 55410, USA
* Corresponding author. Director of Facial Plastic and Reconstructive Surgery, Bobby R. Alford Department of Otorhinolaryngology/Head and Neck Surgery, Baylor College of Medicine, 6550 Fannin, Suite 1701, Houston, TX 77030
E-mail address: [email protected] (A.E. Brissett).
1064-7406/05/$ – see front matter © 2005 Elsevier Inc. All rights reserved.