
Patrick J. Byrne, MD; William E. Walsh, CMI; Peter A. Hilger, MDteven S. Orten, MD
Objective: To evaluate the anatomic effects of the transnasal nasal “inside-out” lateral osteotomy in comparison to a continuous lateral osteotomy to widen the excessively narrow bony nasal pyramid.
Design: A series of 4 fresh cadavers were used. Lateral osteotomies were performed on each cadaver. On one side, a continuous lateral osteotomy was performed with a curved, guarded 4-mm osteotome. On the contralateral side, a straight 2-mm osteotome was used to perform the transnasal perforating inside-out lateral osteotomy. The soft tissue was then dissected off the nasal dorsum and the effects were noted. Specifically, the following factors were assessed: (1) the continuity of the internal and external periosteum; (2) any change, without manipulation, of the position of the lateral nasal walls; (3) the mobility of the fragments; and (4) the effect of any of the preceding factors on the nasal airway.
Results: All 4 cadavers showed identical results. The external and internal periostea were significantly disrupted on each of the sides with continuous osteotomies. The periosteum was completely preserved on the sides, which underwent inside-out lateral osteotomies, with the exception of the 3 or 4 holes created by the 2-mm steotome. In each of the sides with continuous osteotomies, the lateral nasal wall was demonstrably unstable, as the segment was, to varying degrees, displaced inwardly. The inside-out lateral osteotomized segments were uniformly lateralized and stable to gentle palpation. Finally, these changes corresponded to a visible effect on the diameter of the nose in the region of the nasal valve. The inward displacement of the segments undergoing continuous osteotomies narrowed the airway. However, the contralateral inside-out osteotomized segments were lateralized, which widened the diameter of the valve.
Conclusions: The inside-out lateral osteotomy is an effective technique for lateral repositioning of the bony lateral sidewall of the nose. It is reproducible and accurate and appears to provide greater preservation of the periosteal support of the bony segments than a continuous osteotomy. This technique provides a more predictable long-term result, with preservation and/or improvement of the nasal airway. The procedure is ideal for managing the bony nasal segment that needs lateralization, particularly in revision rhinoplasties or after trauma.
Arch Facial Plast Surg. 2003;5:251-255
From the Divisions of Facial Plastic and Reconstructive Surgery, Departments of Otolaryngology–Head and Neck Surgery, Johns Hopkins University School of Medicine,
Baltimore, Md (Dr Byrne), and University of Minnesota, Minneapolis (Dr Hilger).
Mr Walsh is a second-year medical student at
Northwestern University School of Medicine, Chicago, Ill

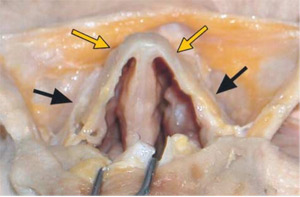
FlG. 1. Planned osteotomies. Continuous high-low-high osteotomy performed on the right side with 4-mm guarded osteotome; transnasal “inside-out” lateral osteotomy performed on the left side.
LATERAL OSTEOTOMY techniques in rhinoplasty have evolved over the years. In 1898, Joseph described his rhinoplasty technique, using a saw to make a low, continuous steotomy. His approach was the most commonly used technique for decades to follow. The reintroduction of chisels occurred during the 1920s and 1930s. Also, there was a greater appreciation of the effects of these osteotomies on both the external aesthetics of the nose and the nasal airway. The low osteotomy was initially replaced with the low-high lateral osteotomy, which resulted in less deformity of the upper nose. In the 1970s, Webster et al2 and Farrior3 introduced the high-low-high osteotomy. This advancement better preserved the airway. Not only was the diameter of the piriform aperture not compromised, the soft tissue attachments of the lateral nasal sidewall were better preserved as well, thus preventing iatrogenic nasal obstruction. Tardy and Denney4 helped popularize the use of the micro-osteotome to more precisely perform osteotomies as well as to minimize the dam- age to both the supportive periosteum and the intranasal mucosa. Other developments include the introduction of various osteotomes, such as the curved guarded osteotome. Additional osteotomy techniques have been introduced. These include the intermediate osteotomy, used to address more severe bony deformities, and the perforating percutaneous technique. A transnasal perforating technique was described as early as 1971.5

FlG. 2. After dissection of soft tissue from the side undergoing continuous lateral osteotomy, the disruption of the periosteal attachments laterally is demonstrated. Note the mobility of the involved segment.
The lateral osteotomy has received attention because of the many challenges this maneuver presents. It is associated with a number of potential problems, including postoperative asymmetry, displacement of a destabilized segment, and collapse of the nasal valve and lateral nasal sidewall. The perforating technique has been noted to provide better preservation of the periosteal attachments laterally.6 The technique preferred by the authors in selected patients requiring lateral displacement of the osseous framework involves a transnasal perforating lateral osteotomy. This “inside- out” lateral osteotomy is performed by making a series of “postage-stamp” osteotomies from inferior to superior. The direction of the force vector is therefore directed laterally, which aids in proper displacement of the bony segment in the desired direction.
The study intent was to investigate the anatomic changes that take place with the inside-out lateral osteotomy and to compare this procedure with a continuous osteotomy.

FlG. 3. A Boies elevator inserted on the side undergoing “inside-out” lateral osteotomy. The periosteum is preserved laterally, and the segment is stable to gentle manipulation.
METHODS
MATERIALS
Fresh human cadavers were used for the study. A curved guarded 4-mm osteotome was used to perform a high-low-high osteotomy on the right side in each cadaver. A straight 2-mm unguarded osteotome was used for the inside-out lateral osteotomy on the left side. Standard surgical instruments were then used to dissect the soft tissue from the nasal dorsum. The dimensions of the nasal airway in the region of the nasal valve were visually inspected by transecting the tissue in the axial plane. Digital photographs were then recorded with a digital camera (Nikon 880).
SURGICAL TECHNIQUE
The continuous high-low-high lateral osteotomy on the right side was performed in a standard fashion. After this procedure, the contralateral inside-out lateral osteotomy was performed (Figure 1). The sites of the perforating osteotomies are along the same path as the continuous osteotomy. In the live patient, the internal surface of the bony pyramid is first injected with 1% lidocaine with 1:100 000 epinephrine along the planned osteotomy site. After adequate time for vasoconstriction, the 2-mm straight osteotome is inserted transnasally and the osteotomies are begun. A series of postage stamp osteotomies are made, beginning inferiorly and proceeding superiorly. Typically, 3 or 4 perforations are required to adequately mobilize the segment. The tip of the osteotome is passed directly through mucosa and the internal periosteum. The contralateral hand is used externally to palpate and control the perforations. The surgeon can palpate the segment being dis- placed laterally by the osteotomies. The periosteum of the external surface of the bone is intended to remain intact. At times, some gentle pressure may be applied with a Boies elevator in the nose for effective mobilization. In this case, the elevator was not used so that the effects of the osteotomies alone could be determined. Before either lateral osteotomy technique was carried out, standard bilateral medial fading osteotomies were performed with a curved unguarded osteotome. No dorsal reduction was performed.
The soft tissue was then dissected from the nasal dorsum. A No. 15 blade was used to incise the midline down the dorsum. Transverse incisions were made superiorly at the radix and inferiorly along the ala. The skin–soft tissue envelope was then carefully dissected from the bony-cartilaginous structures in an “open book” fashion. The condition of the periosteum was noted. The position of the bony and cartilaginous side- walls was noted and compared. Digital photographs were taken of the above findings.
RESULT
The results were identical in each of the 4 cadavers. The periosteum on the right side, which had undergone the continuous osteotomy, was significantly disrupted both internally and externally along the entire length of the osteotomy (Figure 2). In each case, the position of the bony segment was lightly medialized. Also, on palpation of the segment, a significant amount of mobility was obvious on each of the specimens.
FlG. 4. Nasal valve. On the right, after the high-low-high continuous osteotomy and without further manipulation, the subtle narrowing of the nasal valve angle is seen. On the left, the “inside-out” lateral osteotomy has resulted in a widening of the nasal valve angle, again without manipulation.
The results of the left side, on which an inside-out osteotomy was performed, were quite different. In each case, the periosteum along the external surface was intact along the entire length of the osteotomy. The position of the bony segment was slightly lateralized. Palpation with the Boies elevator demonstrated the stability of the bony segment on the left side, being less mobile than the right side (Figure 3). Careful division in the axial plane in the region of the nasal valve revealed a small amount of narrowing on the right side, on which the continuous osteotomy was performed. On the left side (on which the inside-out lateral osteotomy was performed), the angle of the nasal valve was increased (Figure 4).
COMMENT
The lateral osteotomy in rhinoplasty is fraught with potential pitfalls. The technique can be difficult to perform, and reliable long-term results may be unreliable. The lateral osteotomy is the most common cause of post-rhinoplasty asymmetry. It has also been noticed that osteotomies often constrict the nasal airway. The upper lateral cartilages cantilever off the nasal bones, which makes the stability of the result critical not only to the postoperative symmetry but also to function. Collapse of the osteotomized segment can result in concomitant medial displacement of the upper lateral cartilages, narrowing the airway in the upper third as well as at the nasal valve. Excessive pinching in the middle vault may result. The senior author was prompted to use the technique described herein by the anatomic study published by Murakami and Larrabee in 1992. Our anatomic study demonstrates the advantages that the inside-out lateral osteotomy technique can provide for patients who require an increased width of the bony nasal dorsum. These advantages address both the potential problems of postoperative asymmetry and excessive narrowing, as well as iatrogenic nasal obstruction. Therefore, the technique is also effective at addressing these issues in the revision rhinoplasty case or after trauma.
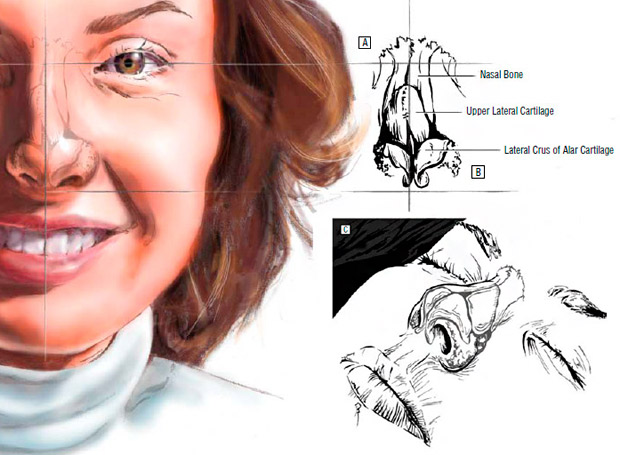
The “inside-out” lateral osteotomy technique is in- tended primarily for the patient with an inwardly dis- placed lateral nasal bony sidewall, a deformity that may be postoperative, posttraumatic, or congenital. The medially displaced nasal bones cause the upper lateral cartilage to be displaced as well, owing to the cantilevered attachment of these cartilages to the undersurface of the nasal bones (Figure 5).
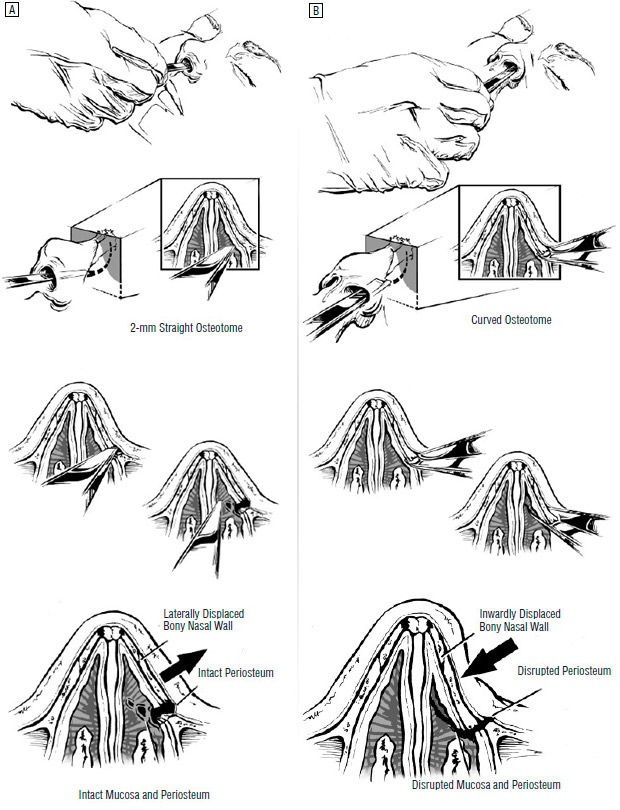
The perforating, postage stamp nature of the technique makes it, in general, less traumatic to the support- ing periosteum than continuous techniques. Greater preservation of periosteal integrity has been noted previously in comparisons of percutaneous perforating osteotomies to continuous techniques in anatomic studies.6 Our findings support the same conclusion for the inside-out lateral osteotomy. The periosteum of the external surface of the osteotomy sites remained intact, which was not the case with the continuous technique (Figure 6); the bony segments were therefore more stable. The ad- vantage of this is obvious: the mobilized segment is less likely to collapse with subsequent healing and contracture of the soft tissue envelope.
There is some obvious mucosal trauma with the inside-out technique. However, continuous techniques have been implicated in mucosal disruption. The percutaneous perforating technique, conversely, has been noted to prevent mucosal trauma. In our experience, this intentional trauma to the intranasal mucosa has not proved clinically significant. Rather than causing a long, continuous area of mucosal disruption, the inside-out technique uses a limited number (3-4) of small (2-mm) perforations. Bleeding, synechia, and other complications have not been noted. Rarely, at the conclusion of the case, a small piece of rolled oxidized cellulose (Surgicel), placed high in the nose and secured with externalized suture, is used to stabilize the segments.
The direction of the force vector producing the osteotomies is important. The direction of force is medial to lateral. Thus, the mobilization of the bony segment tends to follow the same path. Our results confirm the effect of this. The displacement of the osteotomized segments occurred even without manipulation. An obvious improvement in the dimensions of the nasal valve was produced, which makes the technique ideal for patients with bony deviations toward the midline due to trauma or previous rhinoplasty and in the congenitally narrow nose in which some lateral displacement is desired. It follows that this maneuver should not be the procedure of choice for patients in whom a medialization of the bony segment is desired. When a bony segment requires movement toward the midline, a percutaneous perforating osteotomy should be chosen instead.
We have used the inside-out technique for many years in cases involving trauma and in secondary rhinoplasties, with very gratifying results, which have proved to be reliable and long-lasting.
CONCLUSIONS
The osteotomy technique must be chosen to address the specific needs of the patient in each case. It also must be accurate and provide long-term stability. Patients who require lateralization of the bony pyramid of the nose may be served best by the technique described herein. The in- side-out lateral osteotomy is easy to perform, and quite precise. It preserves the periosteal support of the bony framework, which, in conjunction with the direction of force applied, provides for correct, stable positioning of the bony sidewall. This makes this technique a very useful addition to the surgeon’s armamentarium.
Accepted for publication March 28, 2002.
Corresponding author and reprints: Patrick J. Byrne, MD, Division of Facial Plastic and Reconstructive Surgery, Department of Otolaryngology–Head and Neck Surgery, Johns Hopkins University School of Medicine, 601 N Caro- line St, Sixth Floor, Baltimore, MD 21287-1910 (e-mail: [email protected]).
REFERENCES
- Joseph J. Die Hypertrophie der starren Nase: Nasenplastik und sonstige gesichtsplastik über smammaplastik und einige weitere Operationen aus dem gebiete der ausseren Korperplastik. Leipzig, Germany: Kabitzsch; 1931.
- Webster RC, Davidson TM, Smith RC. Curved lateral osteotomy for airway protection in rhinoplasty. Arch Otolaryngol. 1977;103:454-458.
- Farrior RT. The osteotomy in rhinoplasty. Laryngoscope. 1978;88:1449-1459.
- Tardy ME, Denney JC. Micro-osteotomies in rhinoplasty. Facial Plast Surg. 1984; 1:137-145.
- Diamond HP. Rhinoplasty technique. Surg Clin North Am. 1971;51:317-331.
- Murakami C, Larrabee W. Comparison of osteotomy techniques in the treatment of nasal fractures. Facial Plast Surg. 1992;8:209-219.
ARCH FACIAL PLAST SURG/ VOL 5, MAY/JUN 2003 WWW.ARCHFACIAL.COM
Downloaded from archfaci.ama-assn.org at University of Minnesota Twin Cities, on 5 March 2012 ©2003 American Medical Association. All rights reserved